Please review the ACG Clinical Guideline on The Diagnosis and Management of Idiosyncratic Drug-Induced Liver Injury
Idiosyncratic drug-induced liver injury (DILI) is a rare adverse drug reaction and it can lead to jaundice, liver failure, or even death. Antimicrobials and herbal and dietary supplements are among the most common therapeutic classes to cause DILI in the Western world. DILI is a diagnosis of exclusion and thus careful history taking and thorough work-up for competing etiologies are essential for its timely diagnosis. In this ACG Clinical Guideline, the authors present an evidence-based approach to diagnosis and management of DILI with special emphasis on DILI due to herbal and dietary supplements and DILI occurring in individuals with underlying liver disease. Download the Guideline for your review.
Terminology and definitions
Intrinsic DILI – Hepatotoxicity with potential to affect all individuals to varying degrees. Reaction typically stereotypic and dose dependent (e.g., acetaminophen).
Idiosyncratic DILI – Hepatotoxicity affecting only rare susceptible individuals. Reaction less dose dependent and more varied in latency, presentation, and course.
Chronic DILI – Failure of return of liver enzymes or bilirubin to pre-DILI baseline, and/or other signs or symptoms of ongoing liver disease (e.g., ascites, encephalopathy, portal hypertension, coagulopathy) 6 months after DILI onset.
Latency – Time from medication (or HDS) start to onset of DILI.
Wash-out, resolution, or de-challenge – Time from DILI onset to return of enzymes and/or bilirubin to pre-DILI baseline levels.
Rechallenge – Re-administration of medication or HDS to a patient who already had a DILI to the same agent.
Hy’s law – Observation made by late Hyman Zimmerman suggesting a 1 in 10 mortality risk of DILI if the following three criteria are met:
- Serum ALT or AST > 3 × ULN
- Serum total bilirubin elevated to > 2 × ULN, without initial findings of cholestasis (elevated serum alkaline phosphatase)
- No other reason can be found to explain the combination of increased aminotransferases and bilirubin, such as viral hepatitis A, B, C, or other preexisting or acute liver disease
Temple’s corollary – An imbalance in the frequency of ALT > 3 × ULN between active treatment and control arms in a randomized controlled trial. This is used to assess for hepatotoxic potential of a drug from premarketing clinical trials
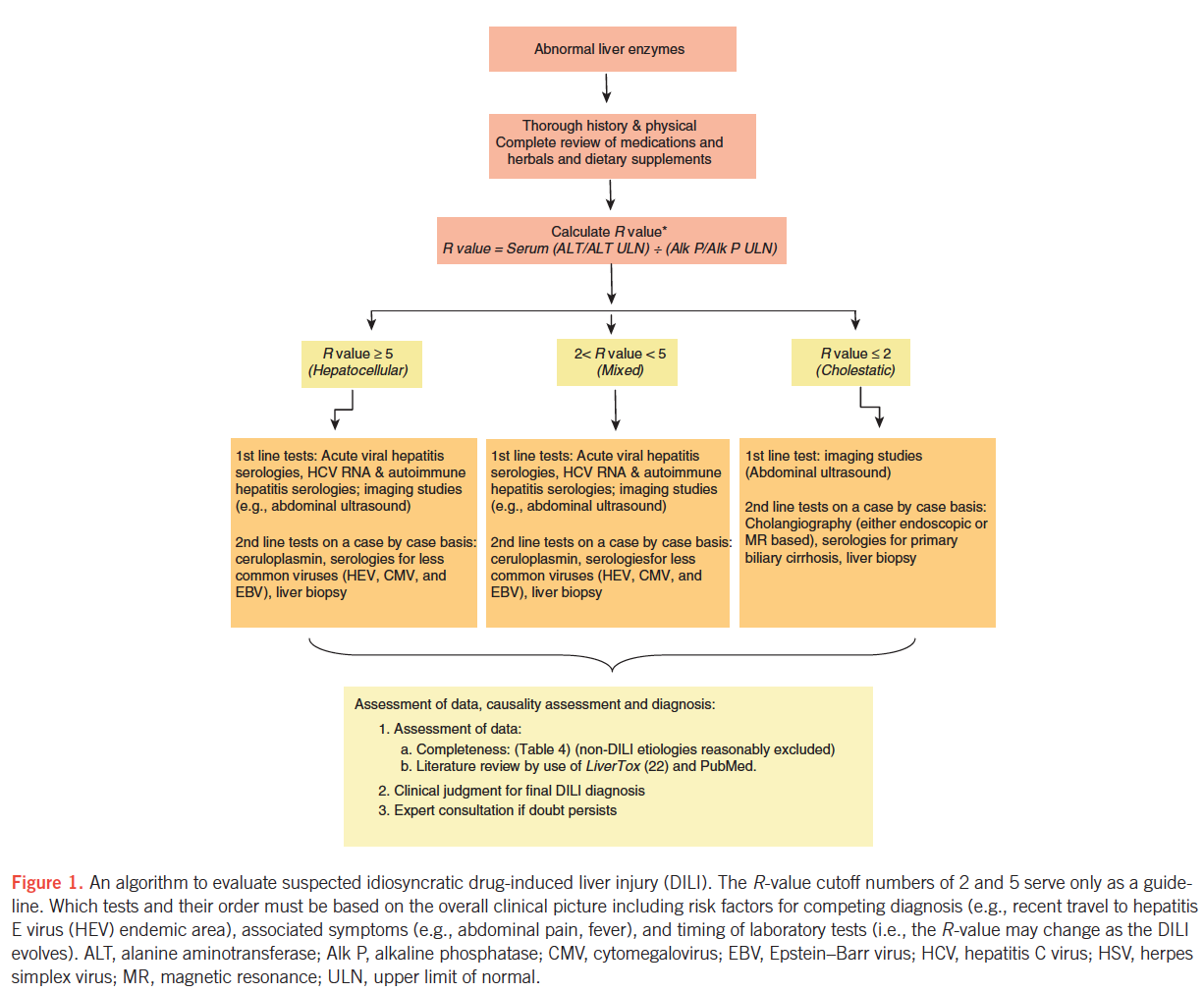
R-value – ALT/ULN ÷ AP/ULN. Used to defined hepatotoxicity injury patterns: hepatocellular (R > 5), mixed (R =2 – 5), and cholestatic (R < 2)
RUCAM – Diagnostic algorithm that uses a scoring system based on clinical data, pre-existing hepatotoxicity literature on the suspected agent and rechallenge
Variables that may predispose individuals to idiosyncratic DILI
- Host factors
- Age
- Gender
- Pregnancy
- Malnutrition
- Obesity
- Diabetes mellitus
- Co-morbidities including underlying liver disease
- Indications for therapy
- Environmental factors
- Smoking
- Alcohol consumption
- Infection and inflammatory episodes
- Drug-related factors
- Daily dose
- Metabolic profile
- Class effect and cross-sensitization
- Drug interactions and polypharmacy
Recommended minimal elements of a diagnostic evaluation in the work-up of suspected DILI
- Gender – Particularly pertinent for competing disorders (e.g., PBC)
- Age – Particularly pertinent for competing disorders (e.g., HEV)
- Race/ethnicity – Particularly pertinent for competing disorders (e.g., sarcoidosis, sickle cell-related biliary stone disease, oriental sclerosing cholangitis)
- Indication for use of drug or herbal or dietary supplement (HDS)
- Concomitant diseases – Particularly pertinent disorders may include sepsis, heart failure, hypotension episodes, recent general anesthesia, parenteral nutrition, and cancer
- Presence of rechallenge – Give timing of rechallenge if done
- History of other drug reactions – Certain cross-reactivities may exist (e.g., anti-epileptics)
- History of other liver disorders – Chronic viral hepatitis, NAFLD, hemochromatosis, alcoholic liver disease, PSC, PBC, liver cancer
- History of alcohol use – Past vs. present; estimated grams per day; sporadic vs. binge drinking vs. regular (daily or weekly)
- Exposure time (“latency”) – Start and stop dates or total number of days, weeks, or months taken
- Symptoms and signs – Presence or absence, time of onset, type (fatigue, weakness, abdominal pain, nausea, dark urine, icterus, jaundice, pruritus, fever, rash)
- Physical findings – Fever, rash, hepatomegaly, hepatic tenderness, signs of chronic liver disease
- Medications and HDS products – Complete list of medications or HDS products with particular attention to those started in the previous 6 months
- Laboratory results – Day of first abnormal liver biochemistry; liver biochemistries, eosinophil counts at presentation
- Viral hepatitis serologies – Anti-HAV IgM, HBsAg, anti-HBc IgM, anti-HCV, HCV RNA
- Auto-immune hepatitis serologies – ANA, anti-smooth muscle antibody, IgG level
- Imaging – US± Doppler, CT, or MRI ± MRCP
- Histology, if available – Timing of biopsy in relation to enzyme elevation and onset
- Washout (de-challenge) data – Follow-up liver biochemistries
- Clinical outcome – Resolution, transplant, death, and timing of each
Most common or well-described DILI agents and the patterns of their liver injury
Agent – Latency – Typical pattern of injury/identifying features (short=3-30 days; moderate=30-90 days; long > 90 days).
- Antibiotics
- Amoxicillin/clavulanate – Short to moderate – Cholestatic injury, but can be hepatocellular; DILI onset is frequently detected after drug cessation
- Isoniazid – Moderate to long – Acute hepatocellular injury similar to acute viral hepatitis
- Trimethoprim/sulfamethoxazole – Short to moderate – Cholestatic injury, but can be hepatocellular; often with immunoallergic features (e.g., fever, rash, eosinophilia)
- Fluoroquinolones – Short – Variable: hepatocellular, cholestatic, or mixed in relatively similar proportions
- Macrolides – Short – Hepatocellular, but can be cholestatic
- Nitrofurantoin
- Acute form (rare) – Short – Hepatocellular
- Chronic form – Moderate to long (months – years) – Typically hepatocellular; often resembles idiopathic autoimmune hepatitis
- Minocycline – Moderate to long – Hepatocellular and often resembles autoimmune hepatitis
- Anti-epileptics
- Phenytoin – Short to moderate – Hepatocellular, mixed, or cholestatic often with immune-allergic features (e.g., fever, rash, eosinophilia) (anti-convulsant hypersensitivity syndrome)
- Carbamazepine – Moderate – Hepatocellular, mixed, or cholestatic often with immune-allergic features (anti-convulsant hypersensitivity syndrome)
- Lamotrigine – Moderate – Hepatocellular often with immune-allergic features (anti-convulsant hypersensitivity syndrome)
- Valproate
- Hyperammonemia – Moderate to long – Elevated blood ammonia, encephalopathy
- Hepatocellular – Moderate to long – Hepatocellular
- Reye-like syndrome – Moderate – Hepatocellular, acidosis; microvesicular steatosis on biopsy
- Analgesics
- Non-steroidal anti-inflammatory agents – Moderate to long – Hepatocellular injury
- Immune modulators
- Interferon-β – Moderate to long – Hepatocellular
- Interferon-α – Moderate – Hepatocellular, autoimmune hepatitis-like
- Anti-TNF agents – Moderate to long – Hepatocellular. Can have autoimmune hepatitis features
- Azathioprine – Moderate to long – Cholestatic or hepatocellular, but can present with portal hypertension (veno-occlusive disease, nodular regenerative hyperplasia)
- Herbals and dietary supplements
- Green tea extract (catechin) – Short to moderate – Hepatocellular
- Anabolic steroids – Moderate to long – Cholestatic; likely contained as adulterants in performance-enhancing products
- Pyrrolizidne alkaloids – Moderate to long – Sinusoidal obstruction syndrome / veno-occlusive disease; contained in some teas
- Flavocoxib – Short to moderate – Mixed hepatocellular and cholestatic
- Miscellaneous
- Methotrexate (oral) – Long – Fatty liver, fibrosis
- Allopurinol – Short to moderate – Hepatocellular or mixed. Often with immune-allergic features. Granulomas often present on biopsy
- Amiodarone (oral) – Moderate to long – Hepatocellular, mixed, or cholestatic. Macrovesicular steatosis and steatohepatitis on biopsy
- Androgen-containing steroids – Moderate to long – Cholestatic. Can present with peliosis hepatis, nodular regenerative hyperplasia, or hepatocellular carcinoma
- Inhaled anesthetics – Short – Hepatocellular. May have immune-allergic features ± fever
- Sulfasalazine – Short to moderate – Mixed, hepatocellular, or cholestatic. Often with immunoallergic features
- Proton pump inhibitors – Short – Hepatocellular; very rare
DILI: Summary statements and recommendations
- Accurate clinical history related to medication exposure and the onset of liver test abnormalities should be obtained when DILI is suspected.
- DILI is a diagnosis of exclusion, and thus appropriate competing etiologies should be excluded in a systematic manner.
- On the basis of the R-value at presentation, DILI can be categorized into hepatocellular, cholestatic, or mixed types. This categorization allows testing for competing etiologies in a systematic approach.
- Liver biopsy can help confirm a clinical suspicion of DILI, provide important information regarding disease severity, and also help exclude competing causes of liver injury.
- In individuals with suspected hepatocellular or mixed DILI:
- Acute viral hepatitis (A, B, and C) and autoimmune hepatitis should be excluded with standard serologies and HCV RNA testing.
- Routine anti-hepatitis E virus IgM testing cannot be recommended owing to unclear performance characteristics of the currently available commercial tests. However, it should be considered in the setting of heightened clinical suspicion (e.g., recent travel in an endemic area).
- Testing for acute cytomegalovirus, acute Epstein-Barr virus, or acute herpes simplex virus infection should be undertaken if classical viral hepatitis has been excluded or clinical features such as atypical lymphocytosis and lymphadenopathy suggest such causes.
- Wilson’s disease and Budd-Chiari syndrome should be considered when clinically appropriate
- In individuals with suspected cholestatic DILI:
- Abdominal imaging (ultrasound or computerized tomography scan) should be performed in all instances to exclude biliary tract pathology and infiltrative processes.
- Serological testing for primary biliary cirrhosis should be limited to those with no evidence of obvious biliary tract pathology on abdominal imaging.
- Endoscopic retrograde cholangiography should be limited to instances where routine imaging is unable to exclude impacted common bile duct stones, primary sclerosing cholangitis, or pancreatico-biliary malignancy.
- When to consider a liver biopsy?
- A liver biopsy should be considered if autoimmune hepatitis remains a competing etiology and if immunosuppressive therapy is contemplated.
- A liver biopsy may be considered in the following situations:
- If there is unrelenting rise in liver biochemistries or signs of worsening liver function despite stopping the suspected off ending agent,
- If the peak alanine aminotransferase level has not decreased by > 50 % at 30 – 60 days aft er the onset in cases of hepatocellular DILI, or if the peak alkaline phosphatase has not fallen by > 50 % at 180 days in cases of cholestatic DILI despite stopping the suspected off ending agent,
- In cases of DILI where continued use or re-exposure to the implicated agent is expected,
- If liver biochemistry abnormalities persist beyond 180 days to evaluate for the presence of chronic liver diseases (CLDs) and chronic DILI.
- In general, outcomes of idiosyncratic DILI are good, with only ~ 10 % reaching the threshold of ALF (coagulopathy and encephalopathy).
- DILI that does evolve to ALF carries a poor prognosis, with 40 % requiring liver transplantation and 42 % dying of the episode. Advanced coma grade and high MELD scores are associated with bad outcomes.
- Prognostic scores to predict outcome for DILI reaching the threshold of ALF are poor or rudimentary.
- Re-exposure to a drug that is thought likely to have caused hepatotoxicity is strongly discouraged, especially if the initial liver injury was associated with significant aminotransferase elevation (for example, > 5xULN, Hy ’ s law, or jaundice). An exception to this recommendation is in cases of life-threatening situations where there is no suitable alternative.
- In individuals with suspected DILI, especially when liver biochemistries are rising rapidly or there is evidence of liver dysfunction, the suspected agent(s) should be promptly stopped.
- No definitive therapies are available either for idiosyncratic DILI with or without ALF: however, NAC may be considered in adults with early-stage ALF, given its good safety profile and some evidence for efficacy in early coma stage patients.
- NAC is not recommended for children with severe DILI leading to ALF
Herbal or dietary supplement (HDS) induced liver injury
- HDS account for an increasing proportion of DILI events in the United States, with body building and weight loss supplements being the most commonly implicated.
- The current regulation for HDS differs substantially from conventional prescription medications. Most importantly, there is no requirement for premarketing safety analyses of HDS.
- Patients and providers must be aware that regulation is not rigorous enough to assure complete safety of marketed products. Patients should be made aware of this fact, and of the potential for HDS to cause liver injury.
- Current causality assessment approaches are not well suited for HDS hepatotoxicity, given the possibility of product variability and contamination; however, expert opinion is probably the best suited for HDS hepatotoxicity, as all information is taken into consideration in assigning a likelihood of injury.
- Voluntary reporting of suspected HDS hepatotoxicity cases through the FDA MEDWATCH system is essential.
- Patients should be encouraged to report the use of HDS to their health-care providers, and be reminded that supplements are not subjected to the same rigorous testing for safety and efficacy as are prescription medications.
- The same diagnostic approach for DILI is applicable to suspected HDS hepatotoxicity. That is, other forms of liver injury must be excluded through a careful history and appropriate laboratory testing and hepatobiliary imaging. Excluding other causes, the diagnosis of HDS hepatotoxicity can be made with confidence in the setting of recent use of HDS.
- Patients with suspected HDS hepatotoxicity should stop all HDS hepatotoxicity and be monitored for resolution of their liver injury.
DILI in patients with chronic liver disease (CLD)
- There are no data to show that underlying CLD is a major risk factor for all-cause DILI, but it may increase the risk for DILI due to selected medications. Patients with chronic HBV and HCV may be more prone to develop liver injury due to specific agents such as isoniazid and antiretrovirals, and may experience more severe outcomes.
- Individuals with underlying fatty liver disease are not at an increased risk for hepatotoxicity from statins.
- The diagnosis of DILI in patients with CLD requires a high index of suspicion and exclusion of other more common causes of acute liver injury, including a flare-up of the underlying liver disease.
- The use of potentially hepatotoxic drugs in CLD patients should be based upon the risk versus benefit of the proposed therapy on a case-by-case basis.
- There are no data to recommend a specific liver biochemistry monitoring plan when a potential hepatotoxic agent is prescribed in individuals with known CLD. Often, information contained in the package inserts is incomplete or unhelpful. Patients should be advised to promptly report any new-onset symptoms such as scleral icterus, abdominal pain / discomfort, nausea / vomiting, pruritis, or choluria. In addition, it is reasonable to monitor serum liver biochemistries at 4 – 6 week intervals, especially during the initial 6 months of treatment with a potentially hepatotoxic agent.
In Summary
- In individuals with suspected hepatocellular or mixed DILI:
- Acute viral hepatitis (A, B, and C) and auto-immune hepatitis should be excluded with standard serologies and HCV RNA testing.
- Anti-HEV IgM testing cannot be recommended because of unclear performance characteristics of the currently available commercial tests. However, it should be considered in the setting of heightened clinical suspicion (e.g., recent travel in an endemic area).
- Testing for acute CMV, acute EBV, or acute HSV infection should be undertaken if classical viral hepatitis has been excluded or clinical features such as atypical lymphocytosis, lymphadenopathy suggest such causes.
- Wilson’s disease and Budd-Chiari syndrome should be considered when clinically appropriate.
- In individuals with suspected cholestatic DILI:
- Abdominal imaging (ultrasound or CT scan) should be performed in all instances to exclude biliary tract pathology and infi ltrative processes.
- Serological testing for primary biliary cirrhosis should be limited to those with no evidence of obvious biliary tract pathology on abdominal imaging.
- Endoscopic retrograde cholangiography should be limited to instances where routine imaging is unable to exclude impacted common bile duct stones, primary sclerosing cholangitis, or pancreatico-biliary malignancy.
- When to consider a liver biopsy?
- A liver biopsy should be considered if autoimmune hepatitis remains a competing etiology and if immunosuppressive therapy is contemplated.
- A liver biopsy may be considered:
- If there is unrelenting rise in liver biochemistries or signs of worsening liver function despite stopping the suspected offending agent.
- If peak ALT level has not fallen by > 50 % at 30 – 60 days after onset in cases of hepatocellular DILI, or if peak Alk P has not fallen by > 50 % at 180 days in cases of cholestatic DILI despite stopping the suspected offending agent.
- In cases of DILI where continued use or re-exposure to the implicated agent is expected.
- If liver biochemistry abnormalities persist beyond 180 days to evaluate for the presence of chronic liver diseases and chronic DILI.
- Re-exposure to a drug thought likely to have caused hepatotoxicity is strongly discouraged, especially if the initial liver injury was associated with significant aminotransferase elevation (e.g., > 5xULN, Hy’s law), or jaundice. An exception to this recommendation is in cases of life-threatening situations where there is no suitable alternative.
- In individuals with suspected DILI, especially when liver biochemistries are rising rapidly or there is evidence of liver dysfunction, suspected agent(s) should be promptly stopped.
- No definitive therapies are available either for idiosyncratic DILI with or without ALF: however, NAC may be considered in adults with early-stage ALF, given its good safety profile and some evidence for efficacy in early coma stage patients.
- NAC is not recommended for children with severe DILI leading to ALF.
- Patients should be encouraged to report use of HDS to their health-care providers, and be reminded that supplements are not subjected to the same rigorous testing for safety and efficacy as are prescription medications.
- The same diagnostic approach for DILI is applicable to suspected HDS-hepatotoxicity. That is, other forms of liver injury must be excluded through a careful history, and appropriate laboratory testing and hepatobiliary imaging. Excluding other causes, the diagnosis of HDS-hepatotoxicity can be made with confidence in the setting of recent use of HDS.
- Patients with suspected HDS-hepatotoxicity should stop all HDS-hepatotoxicity and be monitored for resolution of their liver injury.
- The diagnosis of DILI in patients with CLD requires a high index of suspicion and exclusion of other more common causes of acute liver injury including a flare-up of the underlying liver disease.
- The use of potentially hepatotoxic drugs in CLD patients should be based upon the risk vs. benefit of the proposed therapy on a case-by-case basis.
- There are no data to recommend a specific liver biochemistry monitoring plan when a potential hepatotoxic agent is prescribed in individuals with known CLD. Often, information contained in the package inserts is incomplete or unhelpful. Patients should be advised to promptly report any new onset symptoms such as yellowing of their eyes, abdominal pain / discomfort, nausea / vomiting, itching, or dark urine. In addition, it is reasonable to monitor serum liver biochemistries at 4 – 6 weekly intervals, especially during the initial 6 months of treatment with a potentially hepatotoxic agent.
Am J Gastroenterol advance online publication, 17 June 2014; doi: 10.1038/ajg.2014.131
Abbreviations:
ALF, acute liver failure;
Alk P, alkaline phosphatase;
ALT, alanine aminotransferase;
ANA, anti-nuclear antibody;
AP, alkaline phosphatase;
AST, aspartate aminotransferase;
CLD, chronic liver disease
CMV, cytomegalovirus;
CT, computerized tomography;
DILI, drug-induced liver injury;
EBV, Epstein-Barr virus;
HAV, hepatitis A virus;
HBc, hepatitis B core antigen;
HBs, hepatitis B surface antigen;
HCV, hepatitis C virus;
HDS, herbal or dietary supplement;
HEV, hepatitis E virus;
HSV, herpes simplex virus;
NAC, N-acetyl cysteine:
NAFLD, nonalcoholic fatty liver disease;
PBC, primary biliary cirrhosis;
PSC, primary sclerosing cholangitis;
Ig, immunoglobulin;
MRI, magnetic resonance imaging;
MRCP, magnetic resonance cholangiopancreatography;
RUCAM, Roussel Uclaf Causality Assessment Method;
TNF, tumor necrosis factor;
ULN, upper limit of normal.
US, ultrasound.
