Home » Guidelines
Category Archives: Guidelines
Medical Management of Microscopic Colitis
American Gastroenterological Association Institute Guideline on the Medical Management of Microscopic Colitis
Microscopic colitis presents as chronic watery diarrhea, is diagnosed by mucosal biopsy, and consists of the subtypes lymphocytic colitis and collagenous colitis. Management of the subtypes is similar. This new guideline from the AGA provides medical treatment recommendations and was published online November 13, 2015
Key Recommendations:
For symptomatic microscopic colitis, use budesonide as first-line therapy over mesalamine for induction of remission, and use budesonide for maintenance. During maintenance of remission, budesonide is typically tapered to the lowest effective dose. When budesonide therapy is not feasible, treat patients with mesalamine, bismuth salicylate, or prednisone for induction of remission. For induction of remission, do not treat patients with probiotics or Boswellia serrata, and do not add cholestyramine to mesalamine monotherapy.
Recommendations:
- In patients with symptomatic microscopic colitis, the AGA recommends treatment with budesonide over no treatment for the induction of clinical remission.
- In patients with symptomatic microscopic colitis, the AGA recommends treatment with budesonide over mesalamine for the induction of clinical remission.
- In patients with symptomatic microscopic colitis in whom budesonide therapy is not feasible, the AGA suggests treatment with mesalamine over no treatment for the induction of clinical remission.
- In patients with symptomatic microscopic colitis in whom budesonide therapy is not feasible, the AGA suggests treatment with bismuth salicylate over no treatment for the induction of clinical remission.
- In patients with symptomatic microscopic colitis in whom budesonide therapy is not feasible, the AGA suggests treatment with prednisolone (or prednisone) over no treatment for the induction of clinical remission.
- In patients with symptomatic microscopic colitis, the AGA suggests against combination therapy with cholestyramine and mesalamine over mesalamine alone for the induction of clinical remission.
- A single randomized clinical trial failed to show benefit from the addition of cholestyramine to mesalamine therapy. The AGA considered not only the uncertain balance between benefits and harms but also the feasibility of taking cholestyramine, which can interfere with the administration of other medications, especially in an older population in which polypharmacy is commonplace.
- In patients with symptomatic microscopic colitis, the AGA suggests against treatment with Boswellia serrata over no treatment for the induction of clinical remission.
- In patients with symptomatic microscopic colitis, the AGA suggests against treatment with probiotics over no treatment for the induction of clinical remission.
- For patients with recurrence of symptoms following discontinuation of induction therapy for microscopic colitis, the AGA recommends budesonide for maintenance of clinical remission.
Summary
The recommendations for the medical management of microscopic colitis are intended to reduce practice variation and promote high-value care. The evidence supports the first-line use of budesonide for induction and, when appropriate, maintenance therapy. Because the technical review and guideline focused on treatments assessed in clinical trials, it did not address the full armamentarium of therapies currently used in practice. The effectiveness of lower-cost alternatives such as antidiarrheal agents (eg, loperamide) and cholestyramine monotherapy were not addressed and the role of combination therapies has yet to explored. Due to the absence of clinical trial data, this guideline did not address medical treatment of corticosteroid-refractory microscopic colitis. The guideline suggests that immunosuppressants such as azathioprine and anti–tumor necrosis factor agents may benefit these patients.
http://www.gastro.org/guidelines
http://www.gastrojournal.org/article/S0016-5085(15)01625-X/abstract
http://www.gastrojournal.org/article/S0016-5085(15)01625-X/fulltext
AASLD Guidelines for Treatment of Chronic Hepatitis B
The American Association for the Study of Liver Diseases (AASLD) has released comprehensive guidelines for the treatment of chronic hepatitis B (CHB).
CHB affects more than 240 million people globally, causing significant morbidity and mortality. This document focuses on using antiviral therapy in chronic HBV infection and does not address other related and important issues, such as screening, prevention, and surveillance. For broader issues related to diagnosis, surveillance, and prevention as well as treatment in special populations (e.g., liver transplant recipients) that are not addressed by this guideline, the previous AASLD guideline and recent World Health Organization (WHO) guideline are excellent additional resources.
The AASLD formulated a list of discrete questions that physicians are faced with in daily practice.
These questions were:
- Should adults with immune active CHB be treated with antiviral therapy to decrease liver-related complications?
- Should adults with immune-tolerant infection be treated with antiviral therapy to decrease liver-related complications?
- Should antiviral therapy be discontinued in hepatitis B e antigen (HBeAg)-positive persons who have developed HBeAg seroconversion on therapy?
- Should antiviral therapy be discontinued in persons with HBeAg-negative infection with sustained HBV DNA suppression on therapy?
In HBV-monoinfected persons, does entecavir therapy, when compared to tenofovir therapy, have a different impact on renal and bone health? - Is there a benefit to adding a second antiviral agent in persons with persistent low levels of viremia while being treated with either tenofovir or entecavir?
- Should persons with compensated cirrhosis and low levels of viremia be treated with antiviral agents?
- Should pregnant women who are hepatitis B surface antigen (HBsAg) positive with high viral load receive antiviral treatment in the third trimester to prevent perinatal transmission of HBV?
- Should children with HBeAg-positive CHB be treated with antiviral therapy to decrease liver-related complications?
Natural History in Adults and Children
CHB has been traditionally characterized into four phases, reflecting the dynamic relationship between viral replication and evolution and the host immune response. These phases are of variable duration and not every person infected with CHB will evolve through all phases. Given the dynamic nature of CHB infection, serial monitoring of HBV DNA and alanine aminotransferase (ALT) levels is important to characterize the phase of infection. A single ALT and HBV DNA level are insufficient to assign phase of infection and/or need for treatment. Of note, some persons will be in the “gray zones,” meaning that their HBV DNA and ALT levels do not fall into the same phase. Longitudinal follow-up of ALT and HBV DNA levels and/or assessment of liver histology can serve to clarify the phase of infection.
- Immune-tolerant phase: In this highly replicative/low inflammatory phase, HBV DNA levels are elevated, ALT levels are normal (<19 U/L for females and <30 U/L for males), and biopsies are without signs of significant inflammation or fibrosis. The duration of this phase is highly variable, but longest in those who are infected perinatally. With increasing age, there is an increased likelihood of transitioning from immune-tolerant to the HBeAg-positive immune-active phase.
- HBeAg-positive immune-active phase: Elevated ALT and HBV DNA levels in conjunction with liver injury characterize this phase. Median age of onset is 30 years among those infected at a young age. The hallmark of transition from the HBeAg-positive immune-active to -inactive phases is HBeAg seroconversion. The rate of spontaneous seroconversion from HBeAg to antibody to HBeAg (anti-HBe) is less than 2% per year in children younger than 3 years of age and increases during puberty and among adults to 8% and 12% per year, respectively.
- Inactive CHB phase: In this phase, HBV DNA levels are low or undetectable, ALT levels are normal, and anti-HBe is present. Liver histology shows minimal necroinflammation, but variable fibrosis reflecting previous liver injury during the HBeAg-positive immune-active phase. Among persons who undergo spontaneous HBeAg seroconversion, 67%-80% will continue to remain in the inactive CHB phase. Approximately 4%-20% of inactive carriers have one or more reversions back to HBeAg positive.
- HBeAg-negative immune reactivation phase: Among those who seroconvert from HBeAg to anti-HBe positive, 10%-30% continue to have elevated ALT and high HBV DNA levels, and roughly 10%-20% of inactive carriers may have reactivation of HBV replication and exacerbations of hepatitis after years of quiescence. Most of these persons harbor HBV variants in the precore or core promoter region, and liver histology shows necroinflammation and fibrosis. Persons with HBeAg-negative CHB tend to have lower serum HBV DNA levels than those with HBeAg-positive CHB and are more likely to experience a fluctuating course.
The risk of liver-related complications is variable. Among untreated adults with CHB, the cumulative 5-year incidence of cirrhosis is 8%-20%, and among those with cirrhosis, 5-year cumulative risk of hepatic decompensation is 20%, and risk of HCC is 2%-5%. Viral, host, and environmental factors influence risks of cirrhosis and HCC. HBV DNA levels, ALT levels, and HBeAg status are among the most important determinants of risk of progression to cirrhosis, whereas HBV DNA levels (>2,000 IU/mL), HBeAg status, and cirrhosis are key predictors of HCC risk. A biological gradient of risk has been shown in adults with HBV DNA levels above 2,000 IU/mL; a higher HBV DNA level is associated with progressively higher rates of cirrhosis and HCC.
The initial evaluation of persons with CHB should include
- a thorough history and physical examination
- emphasis on risk factors for coinfection, alcohol use, and family history of HBV infection and liver cancer
- Laboratory tests should include
- assessment of liver disease activity and function
- markers of HBV replication
- tests for coinfection with
- hepatitis C virus (HCV)
- hepatitis delta virus (HDV)
- human immunodeficiency virus (HIV) in those at risk.
Owing to the fluctuating nature of CHB, the accuracy of one high HBV DNA level at a single time point in predicting prognosis is poor and regular monitoring of disease status is imperative to determine need for antiviral therapy. The upper limits of normal (ULNs) for ALT values based on healthy subjects are lower than laboratory values derived from all populations, including those with subclinical liver disease.
Determination of the stage of liver disease is important in guiding antiviral therapy decisions and need for surveillance.
- Liver biopsy provides an assessment of the severity of necroinflammation and fibrosis, rules out other causes of liver disease, and may be especially useful for persons who lack clear-cut indications for treatment. Liver biopsy is regarded as the best method to assess the severity of inflammatory activity and fibrosis,
- Noninvasive methods to assess fibrosis severity are also useful, but:
- Acute-on-chronic exacerbations of hepatitis B may lead to overestimation of fibrosis stage by noninvasive tests, and different cutoffs for significant and advanced fibrosis depending on ALT levels have been proposed.
- Serum markers of fibrosis, such as aspartate aminotransferase (AST)-to-platelet ratio index (APRI), FIB-4, FibroTest, and vibration-controlled transient elastography, have only moderate accuracy in identifying persons with significant fibrosis (fibrosis stage 2 or greater on the Metavir scale), but good diagnostic accuracy in excluding advanced fibrosis and may be useful aids in decision making.
Antiviral Therapy
The goals of antiviral treatment are to decrease the morbidity and mortality related to CHB. The achievement of a sustained suppression of HBV replication has been associated with normalization of serum ALT, loss of HBeAg with or without detection of (anti-HBe), and improvement in liver histology. Historically, the term “cure” was avoided in treatment of CHB, given that persistence of covalently closed circular DNA (cccDNA) in the nucleus of hepatocytes, even in persons with serological markers of resolved infection, poses a lifelong risk for reactivation of infection. However, an immunological cure may be defined by HBsAg loss and sustained HBV DNA suppression and a virological cure defined by eradication of virus, including the cccDNA form. The latter is not currently an attainable goal.
There are six therapeutic agents approved for the treatment of adults with CHB in the United States and five therapeutic agents approved for the treatment of children with CHB. Side effects are more frequent with interferon (IFN) therapy than with nucleos(t)ide analogs (NAs) therapy. Overall, all NAs have an excellent safety profile across a wide spectrum of persons with CHB, including those with decompensated cirrhosis and transplant recipients. For persons with HDV coinfection, the only effective treatment is pegylated interferon (Peg-IFN). For persons with HIV coinfection, treatment of HBV needs to be coordinated with HIV therapy given that several HBV drugs have anti-HIV activity (tenofovir, entecavir, lamivudine, and telbivudine).
The guideline answers the above stated critical questions:
- Should adults with immune active CHB be treated with antiviral therapy to decrease liver-related complications?
- Treatment Intervention: Antiviral therapy
Comparison: No treatment
Outcome: Cirrhosis, decompensation, HCC, death, loss of HBsAg - Recommendations: The AASLD recommends antiviral therapy for adults with immune-active CHB (HBeAg negative or HBeAg positive) to decrease the risk of liver-related complications. The AASLD also recommends Peg-IFN, entecavir, or tenofovir as preferred initial therapy for adults with immune-active CHB.
- Treatment Intervention: Antiviral therapy
- Should adults with immune-tolerant infection be treated with antiviral therapy to decrease liver-related complications?
- Treatment Intervention: Antiviral therapy
Comparison: No treatment
Outcome: Cirrhosis, decompensation, HCC, death, loss of HBsAg - Recommendations: The AASLD recommends against antiviral therapy for adults with immune-tolerant CHB. The AASLD suggests that ALT levels be tested at least every 6 months for adults with immune-tolerant CHB to monitor for potential transition to immune-active or -inactive CHB. The AASLD suggests antiviral therapy in the select group of adults >40 years of age with normal ALT and elevated HBV DNA (≥1,000,000 IU/mL) and liver biopsy showing significant necroinflammation or fibrosis.
- Treatment Intervention: Antiviral therapy
- Should antiviral therapy be discontinued in hepatitis B e antigen (HBeAg)-positive persons who have developed HBeAg seroconversion on therapy?
- Treatment Intervention: Continued antiviral therapy
Comparison: Stopping antiviral therapy
Outcome: Cirrhosis, HCC, reactivation, seroreversion, decompensation, loss of HBsAg - Recommendations: The AASLD suggests that HBeAg-positive adults without cirrhosis with CHB who seroconvert to anti-HBe on therapy discontinue NAs after a period of treatment consolidation. The AASLD suggests indefinite antiviral therapy for HBeAg-positive adults with cirrhosis with CHB who seroconvert to anti-HBe on NA therapy, based on concerns for potential clinical decompensation and death, unless there is a strong competing rationale for treatment discontinuation.
- Treatment Intervention: Continued antiviral therapy
- Should antiviral therapy be discontinued in persons with HBeAg-negative infection with sustained HBV DNA suppression on therapy?
- Treatment Intervention: Continued antiviral therapy
Comparison: Stopping antiviral therapy
Outcome: Reactivation, decompensation, loss of HBsAg - Recommendations: The AASLD suggests indefinite antiviral therapy for adults with HBeAg-negative immune-active CHB, unless there is a competing rationale for treatment discontinuation.
- Treatment Intervention: Continued antiviral therapy
- In HBV-monoinfected persons, does entecavir therapy, when compared to tenofovir therapy, have a different impact on renal and bone health?
- Treatment Intervention: Tenofovir
Comparison: Entecavir
Outcome: Renal function, hypophosphatemia, bone health - Recommendations: The AASLD suggests no preference between entecavir and tenofovir regarding potential long-term risks of renal and bone complications.
- Treatment Intervention: Tenofovir
- Is there a benefit to adding a second antiviral agent in persons with persistent low levels of viremia while being treated with either tenofovir or entecavir?
- Treatment Intervention: Continue therapy
Comparison: Change or switch therapy
Outcome: HBV resistance, clinical flare, decompensation, loss of HBeAg - Recommendations: The AASLD suggests that persons with persistent low-level viremia (<2,000 IU/mL) on entecavir or tenofovir monotherapy continue monotherapy, regardless of ALT. The AASLD suggests one of two strategies in persons with virological breakthrough on entecavir or tenofovir monotherapy: either switch to another antiviral monotherapy with high barrier to resistance or add a second antiviral drug that lacks cross-resistance.
- Treatment Intervention: Continue therapy
- Should persons with compensated cirrhosis and low levels of viremia be treated with antiviral agents?
- Treatment Intervention: Antiviral therapy
Comparison: No treatment
Outcome: Decompensation, HCC, death - Recommendations: The AASLD suggests that adults with compensated cirrhosis and low levels of viremia (<2,000 IU/mL) be treated with antiviral therapy to reduce the risk of decompensation, regardless of ALT level. The AASLD recommends that HBsAg-positive adults with decompensated cirrhosis be treated with antiviral therapy indefinitely regardless of HBV DNA level, HBeAg status, or ALT level to decrease risk of worsening liver-related complications.
- Treatment Intervention: Antiviral therapy
- Should pregnant women who are hepatitis B surface antigen (HBsAg) positive with high viral load receive antiviral treatment in the third trimester to prevent perinatal transmission of HBV?
- Treatment Intervention: Antiviral therapy in third trimester
Comparison: No treatment
Outcome: Cirrhosis, decompensation, HCC, death, loss of HBsAg CHB in the infant, maternal safety, fetal/infant safety - Recommendations: The AASLD suggests antiviral therapy to reduce the risk of perinatal transmission of hepatitis B in HBsAg-positive pregnant women with an HBV DNA level >200,000 IU/mL. The AASLD recommends against the use of antiviral therapy to reduce the risk of perinatal transmission of hepatitis B in the HBsAg-positive pregnant woman with an HBV DNA ≤200,000 IU/mL.
- Treatment Intervention: Antiviral therapy in third trimester
- Should children with HBeAg-positive CHB be treated with antiviral therapy to decrease liver-related complications?
- Treatment Intervention: Antiviral therapy
Comparison: No treatment
Outcome: Cirrhosis, decompensation, HCC, death, HBeAg seroconversion, loss of HBsAg - Recommendations: The AASLD suggests antiviral therapy in HBeAg-positive children (ages 2 to <18 years) with both elevated ALT and measurable HBV DNA levels, with the goal of achieving sustained HBeAg seroconversion. The AASLD recommends against use of antiviral therapy in HBeAg-positive children (ages 2 to <18 years) with persistently normal ALT, regardless of HBV DNA level.
- Treatment Intervention: Antiviral therapy
Summary of Recommendations
- The AASLD recommends antiviral therapy for adults with immune-active CHB (HBeAg negative or HBeAg positive) to decrease the risk of liver-related complications.
- The AASLD recommends Peg-IFN, entecavir, or tenofovir as preferred initial therapy for adults with immune-active CHB.
- The AASLD recommends against antiviral therapy for adults with immune-tolerant CHB.
- The AASLD suggests that ALT levels be tested at least every 6 months for adults with immune-tolerant CHB to monitor for potential transition to immune-active or -inactive CHB.
- The AASLD suggests antiviral therapy in the select group of adults >40 years of age with normal ALT and elevated HBV DNA (≥1,000,000 IU/mL) and liver biopsy showing significant necroinflammation or fibrosis.
- The AASLD suggests that HBeAg-positive adults without cirrhosis with CHB who seroconvert to anti-HBe on therapy discontinue NAs after a period of treatment consolidation.
- The AASLD suggests indefinite antiviral therapy for HBeAg-positive adults with cirrhosis with CHB who seroconvert to anti-HBe on NA therapy, based on concerns for potential clinical decompensation and death, unless there is a strong competing rationale for treatment discontinuation.
- The AASLD suggests indefinite antiviral therapy for adults with HBeAg-negative immune-active CHB, unless there is a competing rationale for treatment discontinuation.
- The AASLD suggests no preference between entecavir and tenofovir regarding potential long-term risks of renal and bone complications.
- The AASLD suggests that persons with persistent low-level viremia (<2,000 IU/mL) on entecavir or tenofovir monotherapy continue monotherapy, regardless of ALT.
- The AASLD suggests one of two strategies in persons with virological breakthrough on entecavir or tenofovir monotherapy: either switch to another antiviral monotherapy with high barrier to resistance or add a second antiviral drug that lacks cross-resistance.
- The AASLD suggests that adults with compensated cirrhosis and low levels of viremia (<2,000 IU/mL) be treated with antiviral therapy to reduce the risk of decompensation, regardless of ALT level.
- The AASLD recommends that HBsAg-positive adults with decompensated cirrhosis be treated with antiviral therapy indefinitely regardless of HBV DNA level, HBeAg status, or ALT level to decrease risk of worsening liver-related complications.
- The AASLD suggests antiviral therapy to reduce the risk of perinatal transmission of hepatitis B in HBsAg-positive pregnant women with an HBV DNA level >200,000 IU/mL.
- The AASLD recommends against the use of antiviral therapy to reduce the risk of perinatal transmission of hepatitis B in the HBsAg-positive pregnant woman with an HBV DNA ≤200,000 IU/mL.
- The AASLD suggests antiviral therapy in HBeAg-positive children (ages 2 to <18 years) with both elevated ALT and measurable HBV DNA levels, with the goal of achieving sustained HBeAg seroconversion.
- The AASLD recommends against use of antiviral therapy in HBeAg-positive children (ages 2 to <18 years) with persistently normal ALT, regardless of HBV DNA level.
Abbreviations
ALT alanine aminotransferase
anti-HBe antibody to HBeAg
anti-HBs antibody to HBsAg
APRI AST-to-platelet ratio index
AST aspartate aminotransferase
cccDNA covalently closed circular DNA
CHB chronic hepatitis B
HBV hepatitis B virus
HCV hepatitis C virus
HCC hepatocellular carcinoma
HIV human immunodeficiency virus
HDV hepatitis delta virus
HBsAg hepatitis B surface antigen
HBeAg hepatitis B e antigen
IFN interferon
NA nucleos(t)ide analog
Peg-IFN pegylated interferon
http://www.aasld.org/sites/default/files/guideline_documents/hep28156.pdf
http://onlinelibrary.wiley.com/doi/10.1002/hep.28156/full
American Gastroenterological Association Institute Guidelines on the Management of Acute Diverticulitis
The American Gastroenterological Association (AGA) Institute has issued updated guidelines regarding the management of acute diverticulitis. Routine use of antibiotics in uncomplicated diverticulitis is not recommended, and selective use is more appropriate. Patients who have not had a recent colon exam require colonoscopy after an episode of acute diverticulitis to rule out the possibility of malignancy.
Patients with a history of acute diverticulitis may benefit from a fiber-rich diet or fiber supplementation, and do not need to avoid nuts, seeds, and popcorn. Patients with a history of acute diverticulitis may safely take aspirin but should avoid non-aspirin NSAIDs. Mesalamine, rifaximin, and probiotics all have no proven benefit after an episode of acute diverticulitis. Patients should be advised to exercise.
Recommendations
The AGA suggests:
- that antibiotics should be used selectively, rather than routinely, in patients with acute uncomplicated diverticulitis.
- that colonoscopy be performed after resolution of acute diverticulitis in appropriate candidates to exclude the misdiagnosis of a colonic neoplasm if a high-quality examination of the colon has not been recently performed.
- against elective colonic resection in patients with an initial episode of acute uncomplicated diverticulitis. The decision to perform elective prophylactic colonic resection in this setting should be individualized.
- a fiber-rich diet or fiber supplementation in patients with a history of acute diverticulitis.
- against routinely advising patients with a history of diverticulitis to avoid consumption of seeds, nuts, and popcorn.
- against routinely advising patients with a history of diverticulitis to avoid the use of aspirin.
- advising patients with a history of diverticulitis to avoid the use of nonaspirin NSAIDs if possible.
- against the use of mesalamine after acute uncomplicated diverticulitis.
- against the use of rifaximin after acute uncomplicated diverticulitis.
- against the use of probiotics after acute uncomplicated diverticulitis.
- advising patients with diverticular disease to consider vigorous physical activity.
Important discussion points:
- Antibiotics:
Until recently, antibiotics have been the cornerstone of treatment of patients with acute diverticulitis. The emerging belief that acute diverticulitis may be more inflammatory than infectious, as well as increasing concerns about the overuse of antibiotics have led to the recommendation of selective and individualized antibiotic use. The current data are of low quality, and recommendations could change as further studies are performed. These recommendations should not be generalized to complicated patients (ie, those with abscesses or fistulas), those with signs of severe infection or sepsis, immunosuppressed patients, or patients with other significant comorbidities.
Furthermore, outpatient management without antibiotics has not been studied. - Colonoscopy:
Observational studies of patients with imaging-proven diverticulitis who subsequently underwent colonoscopy detected a small number of colorectal cancers (15/1000 patients) and advanced adenomas (38/1000 patients). Absence of a mass lesion on CT scan does not exclude the possibility of an underlying colonic neoplasm. Evidence of alternative, non-neoplastic explanations for the index presentation, such as inflammatory bowel disease or ischemic colitis, was either infrequently identified or not reported. Although an increased risk of recurrent diverticulitis or colonic perforation is a concern in patients undergoing colonoscopy after an episode of acute diverticulitis, this was not reported as an adverse event. - Elective Colonic Resection:
Approximately 20% of patients with acute uncomplicated diverticulitis experience a recurrent episode of diverticulitis in the following 5 years. The risk of future diverticular complications and need for emergency surgery among patients treated medically without colonic resection is low (<5%). Approximately 10% of patients with elective sigmoid resection after an episode of acute diverticulitis experience short-term complications of surgery, including wound infection, anastomotic leak, and cardiovascular/thrombotic events. Such postoperative risks are increased in patients older than 65 years of age. Long-term complications of abdominal distention, cramping, altered defecation, and fecal incontinence are reported in 25% of patients after elective surgery. The rates of recurrent diverticulitis appear to be higher in younger patients and the operative risks are lower, but the data do not support elective surgery in this subgroup when presenting with acute uncomplicated diverticulitis.
In conclusion, the AGA states that the management of acute diverticulitis has undergone meaningful changes over the past decade, including more judicious use of antibiotics and surgery as well as preliminary and ongoing investigations into medical therapies to decrease symptoms and reduce recurrence.
http://www.gastro.org/guidelines
http://www.gastrojournal.org/article/S0016-5085(15)01432-8/abstract
http://www.gastrojournal.org/article/S0016-5085(15)01432-8/fulltext
The Role of Upper Gastrointestinal Biopsy to Evaluate Dyspepsia in the Adult Patient in the Absence of Visible Mucosal Lesions
American Gastroenterological Association Institute Guideline on the Role of Upper Gastrointestinal Biopsy to Evaluate Dyspepsia in the Adult Patient in the Absence of Visible Mucosal Lesions
This document presents the official recommendations of the American Gastroenterological Association (AGA) on the role of upper gastrointestinal biopsy to evaluate dyspepsia in the absence of mucosal lesions. The guideline was developed by the AGA’s Clinical Practice Guidelines Committee and approved by the AGA Governing Board.
The authors of these guidelines present evidence-based recommendations for performing biopsies of normal mucosa in patients with dyspepsia who are undergoing EGD. The authors take into consideration the different segments of the upper GI tract as well as patient factors such as immune system status. Please make sure to review the entire paper as linked.
Esophagus:
- In patients undergoing EGD for dyspepsia as the sole indication, the AGA recommends against obtaining routine biopsies of the normal-appearing esophagus or GE junction regardless of immune status.
Stomach:
- In immunocompetent patients undergoing EGD for dyspepsia as the sole indication, the AGA recommends obtaining routine biopsies of the normal appearing gastric body and antrum for the detection of HP infection if the HP infection status is unknown.
- In immunocompromised patients undergoing EGD for dyspepsia as the sole indication, the AGA recommends obtaining routine biopsies of the normal-appearing gastric body and antrum for the detection of HP infection if the HP infection status is unknown.
- When obtaining biopsies from the normal-appearing gastric body and antrum for the detection of HP infection, the AGA suggests following the 5-biopsy Sydney System with all specimens placed in the same jar.
- When biopsies are obtained from the normal-appearing gastric body and antrum for the detection of HP infection, the AGA suggests not obtaining automatic special staining of the specimens.
Duodenum:
- In patients undergoing EGD for dyspepsia as the sole indication, and in the absence of signs or symptoms associated with an increased risk of celiac disease, the AGA suggests not obtaining routine biopsies of the normal-appearing duodenum to detect celiac disease.
- In immunocompromised patients undergoing EGD for dyspepsia as the sole indication, the AGA suggests obtaining routine biopsies of the normal-appearing duodenum for the detection of GVHD in post−allogeneic tissue transplantation patients and for opportunistic infections.
- When biopsies are obtained from the normal-appearing duodenum, the AGA suggests not performing routine special staining of the specimens.
Clarifications:
- The updated Sydney System protocol includes specimens from the lesser and greater curve of the antrum within 2−3 cm of the pylorus, from the lesser curvature of the corpus (4 cm proximal to the angularis), from the middle portion of the greater curvature of the corpus (8 cm from the cardia), and one from the incisura angularis. Although a 3-biopsy protocol (1 each from greater curvature of the corpus and antrum and 1 from incisura) also identifies 100% of HP, equivalency of the 3- vs 5-biopsy protocol cannot be definitively established. Given that the time and cost of specimen preparation and processing from the pathology standpoint are the same for a 3- vs 5-biopsy protocol, a conditional recommendation was made to follow the 5-biopsy protocol.
- Regarding Celiac disease the AGA argues that Celiac disease can be present in patients with endoscopically normal duodenum. The prevalence of biopsy-proven celiac disease among patients with dyspepsia is not significantly different from that in the US general population in which screening for celiac disease is not recommended. One must consider the potential for false-positive biopsy diagnosis in this setting, particularly when only early-grade celiac changes (eg, Marsh I−II) are detected. The AGA argues that this recommendation is primarily dependent on very-low-quality prevalence data, and thus a conditional recommendation is warranted (the possibility exists that the true prevalence of celiac disease among patients presenting with dyspepsia might be higher than what the current literature suggests, this recommendation might need to be updated when higher-quality evidence becomes available). Biopsy of the normal-appearing duodenum might be appropriate in patients who are at high risk for celiac disease, as specified by a previous AGA guideline on the diagnosis and management of celiac disease. If the suspicion for celiac disease is high, biopsies of the normal-appearing duodenum can be of value even if serologies (obtained while the patient is on a gluten-free diet) are negative.
http://www.gastro.org/guidelines/2015/10/19/endoscopic-biopsies
http://www.gastrojournal.org/article/S0016-5085%2815%2901065-3/pdf
Canadian Guidelines for the Medical Management of Ulcerative Colitis in Nonhospitalized Patients
- In patients with mild to moderate active ulcerative proctitis, rectal 5-ASA, at a dosage of 1 g daily, is recommended as first-line therapy to induce symptomatic remission.
- In patients with mild to moderate active left-sided UC, 5-ASA enemas, at a dosage of at least 1 g daily, are recommended as an alternative first-line therapy to induce complete remission.
- In patients with mild to moderate active UC of any disease extent beyond proctitis, an oral 5-ASA preparation, at dosages between 2.0 and 4.8 g/day, is recommended as an alternative first-line therapy to induce complete remission.
- In patients with mild to moderate active UC of any disease extent beyond proctitis, the combination of a rectal and an oral 5-ASA preparation over oral 5-ASA alone is suggested as an alternative first-line therapy to induce complete remission.
- It is recommended that patients with UC be evaluated for lack of symptomatic response to oral/rectal 5-ASA induction therapy in 4 to 8 weeks to determine the need to modify therapy.
- In patients with oral or rectal 5-ASA–induced complete remission of mild to moderate active left-sided UC or proctitis, the same therapy shall be continued to maintain complete remission.
- In patients with oral 5-ASA–induced complete remission of mild to moderate active UC of any disease extent, continued oral therapy of at least 2 g/day is recommended to maintain complete remission.
- In selected 5-ASA–naive patients with UC who have achieved symptomatic remission on oral corticosteroids, an oral 5-ASA preparation of at least 2 g/day is recommended while being assessed for corticosteroid-free complete remission.
- In patients with UC who have failed to respond to oral 5-ASA, switching to another oral 5-ASA formulation to induce remission is not recommended.
- When using oral 5-ASA to induce or maintain complete remission of UC, once-daily dosing is preferred over more frequent dosing.
- In patients with moderate to severe active UC, oral corticosteroids are recommended as first-line therapy to induce complete remission.
- In patients with mild to moderate active UC who fail to respond to 5-ASA therapy, oral corticosteroids are recommended as second-line therapy to induce complete remission.
- In patients with mild to moderate active left-sided UC or proctitis who fail to respond to rectal 5-ASA therapy, rectal corticosteroids are suggested as second-line therapy to induce complete remission.
- In patients with UC, oral corticosteroids are not recommended to maintain complete remission because they are ineffective for this indication and their prolonged use is associated with significant adverse effects.
- In patients with mild to moderate UC of any disease extent, oral budesonide MMX is suggested as an alternative first-line therapy to induce complete remission.
- It is recommended that patients with UC be evaluated for lack of symptomatic response to corticosteroid induction therapy within 2 weeks to determine the need to modify therapy.
- In patients with UC, the use of thiopurine monotherapy to induce complete remission is not recommended.
- In selected patients with UC who have achieved symptomatic remission on oral corticosteroids, thiopurine monotherapy is suggested as an option to maintain complete corticosteroid-free remission.
- In patients with UC, the use of methotrexate monotherapy is not recommended to induce or maintain complete remission.
- In patients with UC who fail to respond to thiopurines or corticosteroids, anti-TNF therapy is recommended to induce complete corticosteroid-free remission.
- Anti-TNF therapy should be combined with a thiopurine or methotrexate rather than used as monotherapy to induce complete remission.
- In patients with UC who are corticosteroid dependent, anti-TNF therapy is recommended to induce and maintain complete corticosteroid-free remission.
- It is recommend that patients with UC be evaluated for lack of symptomatic response to anti-TNF induction therapy in 8 to 12 weeks to determine the need to modify therapy.
- In patients with UC who respond to anti-TNF induction therapy, continued anti-TNF therapy is recommended to maintain complete remission.
- In patients with UC who have a suboptimal response to anti-TNF induction therapy, dose intensification is recommended to achieve complete remission.
- In patients with UC who lose response to anti-TNF maintenance therapy, optimizing dose is recommended to recapture complete remission.
- Dose optimization for patients with UC thjrough therapeutic drug monitoring is recommended.
- In patients with primary failure to an anti-TNF therapy, switching to vedolizumab is recommended over switching to another anti-TNF therapy to induce complete corticosteroid-free remission.
- In patients with secondary failure to an anti-TNF therapy, switching to another anti-TNF therapy or vedolizumab is recommended based on therapeutic drug monitoring results to induce complete corticosteroid-free remission.
- In patients with moderate to severe active UC who fail to respond to corticosteroids, thiopurines, or anti-TNF therapies, vedolizumab is recommended to induce complete corticosteroid-free remission.
- Patients with UC shall be evaluated for lack of symptomatic response to vedolizumab induction therapy in 8 to 14 weeks to determine the need to modify therapy.
- In patients with UC who respond to vedolizumab, continued vedolizumab therapy is recommended to maintain complete corticosteroid- free remission.
- Fecal microbial transplant to induce or maintain complete remission in patients with UC is not recommended outside the setting of a clinical trial.
- In patients with UC, probiotics to induce or maintain complete remission outside the setting of a clinical trial are not recommended.
- 5-ASA failure: Inability of the patient to achieve and maintain complete corticosteroid-free remission despite optimal treatment with oral, rectal, or combination 5-ASA therapy
- Thiopurine failure: Inability of the patient to maintain corticosteroid-free complete remission despite dose optimization
- Biologic failure:
- Primary failure: Inability of the patient to achieve corticosteroid-free complete remission despite dose optimization
- Secondary failure: Inability of the patient to maintain corticosteroid-free complete remission after achieving a symptomatic response
- High disease activity (in acute setting)
- Frequency of hospitalization
- Need for surgery
- Inability to work or participate in leisure activities
- Failure to respond to medication
- Complete remission: Both symptomatic remission and endoscopic healing as defined below
- Endoscopic healing: Normal mucosa, vascular blurring, or chronic changes (eg, inflammatory polyps, scarring) without friability
- Symptomatic remission: Normal stool frequency ( 3/day) and no blood in the stool
- Symptomatic response: Meaningful improvement in symptoms as judged by both the patient and physician in the absence of remission; response should not be considered a desirable final outcome but is useful to assess early response to treatment
- Disease Extent
- The extent of endoscopic disease was categorized as
- proctitis (distal to the rectosigmoid junction or within 18 cm of the anal verge)
- left-sided colitis (extending anywhere from the sigmoid to the splenic flexure), or
- extensive colitis (extending beyond the splenic flexure).
- The extent of endoscopic disease was categorized as
- Disease Activity
- Disease activity is best determined by clinical symptoms and an objective assessment of disease activity through endoscopy. Yet is often necessary to make clinical decisions based on symptoms alone. Ideally, a formal scoring tool such as the Mayo score or a similar disease activity score should be used to determine disease activity in patients with UC. The Mayo score includes 4 measures: stool frequency, rectal bleeding, endoscopic findings, and the physician’s global assessment. Although such a scoring system is desirable for accurate and consistent assessment of disease activity, it is often necessary to make management decisions in the absence of endoscopic information while considering the subjective aspects of disease presentation not captured by the full Mayo score. In such circumstances, the partial Mayo score (which omits the endoscopic subscore) can be informative.
- 0 – Normal number of stools for this patient
- 1 – 1–2 stools more than normal
- 2 – 3–4 stools more than normal
- 3 – 5 or more stools more than normal
- 0 – No blood seen
- 1 – Streaks of blood with stool less than half the time
- 2 – Obvious blood with stool most of the time or more
- 3 – Blood passed alone
- 0 – Normal or inactive disease
- 1 – Mild disease (erythema, decreased vascular pattern, mild friability)
- 2 – Moderate disease (marked erythema, absent vascular pattern, friability, erosions)
- 3 – Severe disease (spontaneous bleeding, ulceration)
- 0 – Normal (there are no symptoms of colitis, the patient feels well, and the flexible proctosigmoidoscopy score is 0) (stool frequency = 0; rectal bleeding = 0; patient’s functional assessment = 0; flexible proctosigmoidoscopy findings = 0)
- 1 – Mild disease (mild symptoms and proctoscopic findings that were mildly abnormal) (the subscores should be mostly 1: stool frequency = 0 or 1; rectal bleeding = 0 or 1; patient’s functional assessment = 0 or 1; flexible proctosigmoidoscopy findings = 0 or 1)
- 2 – Moderate disease (more serious abnormalities and proctosigmoidoscopic and symptom scores of 1 or 2) (the subscores should be mostly 2: stool frequency = 1 or 2; rectal bleeding = 1 or 2; patient’s functional assessment = 1 or 2; flexible proctosigmoidoscopy findings = 1 or 2)
- 3 – Severe disease (the proctosigmoidoscopic and symptom scores are 2 to 3 and the patient probably requires corticosteroid therapy and possibly hospitalization) (the subscores should be mostly 3: stool frequency = 2 or 3; rectal bleeding = 2 or 3; patient’s functional assessment = 2 or 3; flexible proctosigmoidoscopy findings = 2 or 3)
- 0 – Generally well
- 1 – Fair
- 2 – Poor
- 3 – Terrible



Upper Endoscopy for Gastroesophageal Reflux Disease – ACP Guidelines
Upper Endoscopy for Gastroesophageal Reflux Disease: Best Practice Advice From the Clinical Guidelines Committee of the American College of Physicians (ACP)
Nearly 38% of the upper endoscopies performed in outpatients with gastroesophageal reflux disease and low-risk dyspepsia do not adhere to current best-practice guidelines. The most common inappropriate uses were in patients who received an inadequate course of proton pump inhibitors (PPIs) before upper endoscopy and in those who underwent too-frequent surveillance of Barrett’s esophagus. Inappropriate use of endoscopy generates unnecessary costs and exposes patients to harms without improving outcomes.
Read the full text here and download the paper. http://annals.org/article.aspx?articleid=1470281
Best Practice Advice
- Upper endoscopy is indicated in men and women with heartburn and alarm symptoms (dysphagia, bleeding, anemia, weight loss, and recurrent vomiting).
- Upper endoscopy is indicated in men and women with:
- Typical GERD symptoms that persist despite a therapeutic trial of 4 to 8 weeks of twice-daily proton-pump inhibitor therapy.
- Severe erosive esophagitis after a 2-month course of proton-pump inhibitor therapy to assess healing and rule out Barrett esophagus. Recurrent endoscopy after this follow-up examination is not indicated in the absence of Barrett esophagus.
- History of esophageal stricture who have recurrent symptoms of dysphagia.
- Upper endoscopy may be indicated:
- In men older than 50 years with chronic GERD symptoms (symptoms for more than 5 years) and additional risk factors (nocturnal reflux symptoms, hiatal hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat) to detect esophageal adenocarcinoma and Barrett esophagus.
- For surveillance evaluation in men and women with a history of Barrett esophagus. In men and women with Barrett esophagus and no dysplasia, surveillance examinations should occur at intervals no more frequently than 3 to 5 years. More frequent intervals are indicated in patients with Barrett esophagus and dysplasia.
GERD, Barrett Esophagus, and Esophageal Adenocarcinoma
Tissue injury is not necessary to fulfill disease criteria, as 50% to 85% of patients with GERD have nonerosive reflux disease. As many as 40% of U.S. adults report some symptoms of reflux (heartburn and regurgitation), and 10% to 20% have symptoms on a weekly or more frequent basis. Approximately 10% of patients with chronic heartburn symptoms have Barrett esophagus. GERD and Barrett esophagus are associated with an increased risk for esophageal adenocarcinoma. While the absolute risk for adenocarcinoma of the esophagus in the general population remains low (26 cases per 1 million in the U.S. population), its incidence has increased more than 5-fold in the past 40 years. Adenocarcinoma of the esophagus carries a poor prognosis with a 5-year survival rate less than 20%. Given the rising prevalence of chronic GERD, the use of upper endoscopy for GERD indications is rising in an effort to promote early detection and reduce the risk for death from adenocarcinoma of the esophagus. Since 1% to 5% of the U.S. adult population may have Barrett esophagus, the public health and financial implications of endoscopic screening and surveillance programs are substantial.
All 3 major U.S. gastroenterologic professional societies have released guidelines but differ in recommendations.
- The American Society of Gastrointestinal Endoscopy (ASGE) recommends that screening upper endoscopy be considered in selected patients with chronic, longstanding GERD:
- Frequent GERD symptoms (several times per week),
- Chronic GERD symptoms (symptoms for >5 years)
- Age > 50 years
- White race
- Male sex
- Nocturnal reflux symptoms
- The American Gastroenterological Association (AGA) guidelines recommend against screening the general population with GERD for Barrett esophagus and esophageal adenocarcinoma but should be considered in patients with GERD who have several risk factors associated with esophageal adenocarcinoma
- Age 50 years or older
- Male sex
- White race
- Hiatal hernia
- Elevated body mass index
- Intra-abdominal distribution of fat
- The American College of Gastroenterology (ACG) guidelines note that screening for Barrett’s esophagus in the general population cannot be recommended at this time. The use of screening in selective populations at higher risk remains to be established, and therefore should be individualized.
- GERD symptoms
- Body mass index
Formulation of these guidelines was hampered by the generally poor quality of data about the use of endoscopic screening and surveillance programs. In many cases, expert opinion formed the basis for specific recommendations.
The value of endoscopy is well-substantiated in several clinical settings.
- GERD associated with the alarm symptoms of dysphagia, bleeding, anemia, weight loss, or recurrent vomiting merits investigation with upper endoscopy because of its yield of potentially clinically actionable findings, such as cancer of the esophagus or stomach, bleeding lesions in the foregut, or stenosis of the esophagus or pylorus.
- Patients with a documented history of severe erosive esophagitis (grade B or worse on a validated A-to-D scoring system) treated with PPIs have a substantial rate of incomplete healing with medical therapy and may have Barrett esophagus in the areas of previously denuded esophageal epithelium. For these reasons, follow-up upper endoscopy is recommended after 8 weeks of PPI therapy for severe esophagitis to ensure healing and to rule out Barrett esophagus.
- The use of upper endoscopy in patients with esophageal stricture secondary to GERD is largely symptom-based. Because recurrence of strictures is common, repeated upper endoscopy with dilatation may be required.
- Screening intervals for patients with Barrett esophagus without dysplasia are recommended at 3- to 5-year intervals. More frequent endoscopy is reserved for the subset of patients who develop low- or high-grade dysplasia, as they face a higher risk for progression to cancer.
- In patients with chronic GERD whose initial endoscopic screening results were negative, no additional endoscopic screening is necessary, even if the patient continues medical therapy. Observational data show that the likelihood of development of Barrett esophagus in the 5 years after a negative result in such patients is less than 2%. Therefore, routine serial endoscopy in patients with initially negative results for Barrett esophagus is not recommended. Patient and primary caregiver expectations may promote overuse as patients may anticipate serial cancer screening and may inappropriately view no screening or a once-in-a-lifetime screening upper endoscopy for GERD symptoms as inadequate. Patients who have Barrett esophagus and no dysplasia may be dissatisfied with a 3- to 5-year interval of surveillance examinations, as patients with Barrett esophagus grossly overestimate their risk for esophageal cancer.
Summary of the ACP best practice advice:
The ACP has found evidence that upper endoscopy is indicated in patients with heartburn and alarm symptoms, such as dysphagia, bleeding, anemia, weight loss, and recurrent vomiting. However, upper endoscopy is not an appropriate first step in most patients with GERD symptoms and is indicated only when empirical PPI therapy for 4 to 8 weeks is unsuccessful. Upper endoscopy is not indicated in asymptomatic patients with a history of esophageal stricture but is appropriate in patients with recurrent symptoms of dysphagia. Screening upper endoscopy should not be routinely done in women of any age or in men younger than 50 years regardless of GERD symptoms because the incidence of cancer is very low in these populations. Screening endoscopy may be indicated in men older than 50 years with several risk factors for Barrett esophagus. This screening decision should include an assessment of the patient’s life-limiting comorbid conditions. Risk factors include chronic GERD symptoms (symptoms of >5 years’ duration), nocturnal reflux symptoms, hiatal hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat. If an initial screening examination is negative for Barrett esophagus or esophageal adenocarcinoma, recurrent periodic endoscopy is not indicated. Among patients found to have Barrett esophagus on screening upper endoscopy, endoscopic surveillance may be indicated at 3- to 5-year intervals. More frequent endoscopic examinations are reserved for patients with low- or high-grade dysplasia because of their higher risk for progression to cancer.
Unnecessary endoscopy exposes patients to preventable harms, may lead to additional unnecessary interventions, and results in unnecessary costs. Patient education strategies should be used to inform patients about current and effective standards of care.

Diagnosis and Management of Asymptomatic Neoplastic Pancreatic Cysts
The American Gastroenterological Association Institute Guideline on the Diagnosis and Management of Asymptomatic Neoplastic Pancreatic Cysts
- The AGA suggests that patients with pancreatic cysts less than 3 cm without a solid component or a dilated pancreatic duct undergo MRI for surveillance in 1 year and then every 2 years for a total of 5 years if there is no change in cyst size or characteristics.
- The AGA suggests that pancreatic cysts with at least 2 high-risk features such as size ≥3 cm, a dilated main pancreatic duct, or the presence of an associated solid component, should be examined with endoscopic ultrasonography-guided fine-needle aspiration (EUS-FNA). The relative increase in risk of malignancy in the presence of high-risk features may be substantial but because the baseline risk is so low, the absolute effect of these features is modest.
- The AGA suggests that patients without concerning EUS-FNA results should undergo MRI surveillance after 1 year and then every 2 years to ensure no change in risk of malignancy. The negative predictive value of unremarkable EUS-FNA results is very high and this in a setting with a very low risk of associated malignancy.
- The AGA suggests that significant changes in the characteristics of the cyst including the development of a solid component, increasing size of the pancreatic duct, and/or diameter ≥3 cm, are indications for EUS-FNA.
- The AGA suggests against continued surveillance of pancreatic cysts if there has been no significant change in the characteristics of the cyst after 5 years of surveillance or if the patient is no longer a surgical candidate.
- The AGA suggests that patients with both a solid component and a dilated pancreatic duct and/or concerning features on EUS and FNA should undergo surgery to reduce the risk of mortality from carcinoma. Surgery is likely to be most beneficial in cases of cyst resection of high-grade dysplasia, thereby preventing malignancy. Since it is clear from other cancers that not all high-grade dysplasia progress, the proportion of patients who truly benefit from surgery is unclear even in this high-risk group.
- The AGA recommends that if surgery is considered for a pancreatic cyst, patients are referred to a center with demonstrated expertise in pancreatic surgery.
- The AGA suggests that patients with invasive cancer or dysplasia in a cyst that has been surgically resected should undergo MRI surveillance of any remaining pancreas every 2 years.
- The AGA recommends against routine surveillance of pancreatic cysts without high-grade dysplasia or malignancy at surgical resection.
- The AGA recommends that before starting any pancreatic cyst surveillance program, patients should have a clear understanding of programmatic risks and benefits.
- Managing Pancreatic Cysts: Less Is More?
- Management of Pancreatic Cysts: The Evidence Is Not Here Yet.
- Management of Pancreatic Cysts in an Evidence-Based World.
- The AGA recommends that before starting any pancreatic cyst surveillance program, patients should have a clear understanding of programmatic risks and benefits.
- The AGA suggests that patients with pancreatic cysts less than 3 cm without a solid component or a dilated pancreatic duct undergo MRI for surveillance in 1 year and then every 2 years for a total of 5 years if there is no change in size or characteristics.
- The AGA suggests that pancreatic cysts with at least 2 high-risk features, such as size ‡3 cm, a dilated main pancreatic duct, or the presence of an associated solid component, should be examined with EUS-FNA.
- The AGA suggests that patients without concerning EUS-FNA results should undergo MRI surveillance after 1 year and then every 2 years to ensure no change in risk of malignancy.
- The AGA suggests that significant changes in the characteristics of the cyst, including the development of a solid component, increasing size of the pancreatic duct, and/or diameter ‡3 cm, are indications for EUS-FNA.
- The AGA suggests against continued surveillance of pancreatic cysts if there has been no significant change in the characteristics of the cyst after 5 years of surveillance or if the patient is no longer a surgical candidate.
- The AGA suggests that patients with both a solid component and a dilated pancreatic duct and/or concerning features on EUS and FNA should undergo surgery to reduce the risk of mortality from carcinoma.
- The AGA recommends that if surgery is considered for a pancreatic cyst, patients are referred to a center with demonstrated expertise in pancreatic surgery.
- The AGA suggests that patients with invasive cancer or dysplasia in a cyst that has been surgically resected should undergo MRI surveillance of any remaining pancreas every 2 years.
- The AGA suggests against routine surveillance of pancreatic cysts without high-grade dysplasia or malignancy at surgical resection.
ACG Clinical Guideline: Primary Sclerosing Cholangitis
- Differential diagnosis of primary sclerosing cholangitis
- Secondary sclerosing cholangitis
- Cholangiocarcinoma
- IgG4-associated cholangitis
- Histiocytosis X
- Autoimmune hepatitis
- HIV syndrome
- Bile duct strictures
- Cholendocholithiasis
- Primary biliary cirrhosis
- Papillary tumors
- Diagnosis
- Endoscopic retrograde cholangiopancreatography (ERCP) has been the most common procedure in diagnosing PBS. However, magnetic resonance cholangiopancreatography (MRCP) is rapidly becoming the preferred method because it is noninvasive, cheaper and has no associated risk of pancreatitis. A liver biopsy is not needed unless a patient is suspected of having small duct PSC.
- Therapy
- There is currently no established treatment for PSC. However, clinicians are using doses of ursodeoxycholic acid at 20 mg/kg per day for treating PSC.
- Endoscopic Management
- Endoscopic treatment of dominant strictures may improve prognosis, help to relieve the complications of pruritus and cholangitis, allow for early diagnosis of cholangiocarcinoma and may lead to improved survival. ERCP with balloon dilatation is recommended for relieving symptoms of dominant strictures of PSC patients. If a PSC patient undergoes ERCP, antibiotic prophylaxis should be taken to prevent post-ERCP cholangitis. Routine stenting after dilation is not recommended.
- IBD and PSC
- Up to 80% of patients with PSC have IBD. Undergoing annual colon surveillance is recommended in PSC patients with colitis at the time of PCS diagnosis. A colonoscopy with biopsies is recommended in PSC patients whether or not there are symptoms at PSC diagnosis. An exam every 3-5 years is also recommended for patients without prior evidence of colitis.
- Hepatobiliary Malignancies and Gallbladder Disease
- PSC patients are at risk for developing hepatobiliary malignancies. The risk for cholangiocarcinoma is several hundred times higher in patients with PSC vs. patients without PSC. Screening for cholangiocarcinoma with regular cross-sectional imaging with ultrasound or magnetic resonance and serial CA 19-9 is recommended every 6 to 12 months. Patients with PSC with gallbladder polyps more than 8 mm should also undergo cholecystectomy.
- Special Situations
- Every PSC patient is unique and some patients may develop autoimmune hepatitis and other infections. Testing for autoimmune hepatitis is recommended for patients with PSC under 25 years of age and for those patients with higher than expected aminotransferases. MRCP is recommended for PSC patients under 25 years of age with autoimmune hepatitis who have elevated alkaline phosphatase serum levels.
- General Management
- Patients with PSC should undergo bone mineral density screening at diagnosis using duel energy X-ray absorption repeated at 2- to 4-year intervals; patients with advanced liver disease should be checked and monitored for fat-soluble vitamin deficiencies; and patients with PSC and mild pruritus should undergo local skin treatment with antihistamines or emollients to reduce symptoms.
- MRCP is preferred over endoscopic retrograde cholangiopancreatography (ERCP) to establish a diagnosis of PSC.
- Liver biopsy is not necessary to make a diagnosis in patients with suspected PSC based on diagnostic cholangiographic findings.
- Liver biopsy is recommended to make a diagnosis in patients with suspected small duct PSC or to exclude other conditions such as suspected overlap with autoimmune hepatitis.
- Antimitochondrial autoantibody testing can help exclude primary biliary cirrhosis.
- Patients with PSC should be tested at least once for elevated serum immunogloblulin G4 (IgG4) levels.
- At this time, there is no established medical treatment for patients with PSC.
- Ursodeoxycholic acid (UDCA) in doses >28 mg/kg/day should not be used for the management of patients with PSC.
- Other treatments that have been tested without any obvious proven clinical benefit or improvement of liver biochemistries include:
- Azathioprine
- Budesonide
- Docosahexaenoic acid
- Methotrexate
- Metronidazole
- Minocycline
- Mycophenolate mofetil
- Nicotine
- Pentoxifylline
- Pirfenodone
- Prednisolone
- Tacrolimus
- Vancomycin
- ERCP with balloon dilatation is recommended for PSC patients with dominant stricture and pruritus, and/or cholangitis, to relieve symptoms.
- PSC with a dominant stricture seen on imaging should have an ERCP with cytology, biopsies, and fluorescence in-situ hybridization (FISH), to exclude diagnosis of cholangiocarcinoma.
- PSC patients undergoing ERCP should have antibiotic prophylaxis to prevent post-ERCP cholangitis.
- Routine stenting after dilation of a dominant stricture is not required, whereas short-term stenting may be required in patients with severe stricture.
- Percutaneous cholangiography for treatment of dominant strictures can be performed in PSC patients with altered anatomy that prevents successful ERCP, such as Roux-en-Y choledo-chojejunostomy or gastric bypass, or as a rescue therapy after failed endoscopic access. Percutaneous cholangiography is generally the second line of treatment after ERCP because of the risk of complications, including hepatic arterial injury, hemobilia, and cholangitis
- Liver transplantation, when possible, is recommended over medical therapy or surgical drainage in PSC patients with decompensated cirrhosis, to prolong survival.
- Patients should be referred for liver transplantation when their Model for End-Stage Liver Disease (MELD) score exceeds 14.
- In specific clinical circumstances, patients with PSC may be offered additional MELD points, to improve their priority for receiving a donor organ for liver transplantation. MELD exception points can be approved by the United Network for Organ Sharing Regional Review Board for the following indications:
- Recurrent episodes of cholangitis, with >2 episodes of bacteremia or >1 episode of sepsis.
- Cholangiocarcinoma less then 3 cm in diameter, without evidence of metastasis, undergoing treatment through an institutional review board-approved clinical trial.
- Intractable pruritus.
- Recurrence of PSC after liver transplantation is relatively common, affecting as many as 20% of patients at 5 years after transplantation.
- The risk of colorectal dysplasia and cancer is significantly higher (approximately four- to fivefold) among patients with PSC and IBD compared with those with IBD without PSC.
- Annual colon surveillance preferably with chromoendoscopy is recommended in PSC patients with colitis beginning at the time of PSC diagnosis.
- A full colonoscopy with biopsies is recommended in patients with PSC regardless of the presence of symptoms to assess for associated colitis at time of PSC diagnosis.
- Some advocate repeating the exam every 3–5 years in those without prior evidence of colitis.
- Consider screening for cholangiocarcinoma with regular cross-sectional imaging with ultrasound or MR and serial CA 19-9 every 6–12 months.
- Cholecystectomy should be performed for patients with PSC and gallbladder polyps >8 mm, to prevent the development of gallbladder adenocarcinoma.
- PSC and autoimmune hepatitis may co-exist in the same patient and the prevalence of autoimmune hepatitis in patients with PSC is ~10%.
- Further testing for autoimmune hepatitis is recommended for patients with PSC <25 years of age or those with higher- than-expected levels of aminotransferases usually 5× upper limit of normal.
- MRCP is recommended for patients <25 years of age with autoimmune hepatitis, who have elevated serum ALP usually greater than 2× the upper limit of normal.
- PSC appears to be much less common among children than adults, with an estimated prevalence 20% lower than in adults and is a rare indication for liver transplantation in this population. PSC in children is more often associated with higher serum aminotransferase levels and concomitant autommune hepatitis, and sclerosing cholangitis is a more common phenomenon, leading to the use of the term “autoimmune sclerosing cholangitis.” Serum ALP may be elevated in children due to bone growth; hence, suspected cholestasis should be confirmed by measurement of gamma-glutamyl transpeptidase levels. Cholangiocarcinoma appears to be rare in this population and surveillance for gallbladder cancer or cholangiocarcinoma is not recommended.
- IgG4-associated pancreatitis and cholangitis is being increasingly recognized in patients who present with sclerosing cholangitis. IgG4-associated autoimmune pancreatitis is a clearly described entity characterized by strictures in the pancreatic duct, elevated IgG4 levels and response to immunosuppressive therapy. This condition may be associated with biliary strictures and elevated plasma IgG4 levels, and liver biopsy may reveal a lymphoplasmacytic infiltrate . In some cases, the biliary disease is predominant and features of autoimmune pancreatitis may or may not be present.
- Measurement of IgG4 levels is reasonable in patients with PSC and consideration should be given to imaging for autoimmune pancreatitis and the presence of IgG4-associated cholangitis among those with markedly elevated IgG4 levels.
- Liver biopsy should be considered to identify the classical lymphoplasmacytic infiltrate and consideration of immunosuppression therapy may be useful in such patients, especially if they have higher-than- expected elevations of serum aminotransferase levels.
- Local skin treatment should be performed with emollients and/or antihistamines in patients with PSC and mild pruritus, to reduce symptoms.
- Bile acid sequestrants such as cholestyramine should be taken (prescribed) in patients with PSC and moderate pruritus to reduce symptoms. Second-line treatment such as rifampin and naltrexone can be considered if cholestyramine is ineffective or poorly tolerated.
- Recommend screening for varices in patients with signs of advanced disease with platelet counts <150×103/dl.
- Patients with PSC should undergo bone mineral density (BMD) screening at diagnosis with dual energy X-ray absorption at diagnosis and repeated at 2- to 4-year intervals.
- Patients with advanced liver disease should be screened and monitored for fat-soluble vitamin deficiencies.
- MRCP is preferred over ERCP to establish a diagnosis of PSC.
- Liver biopsy is not necessary to make a diagnosis in patients with suspected PSC based on diagnostic cholangiographics findings.
- Liver biopsy is recommended to make a diagnosis in patients with suspected small duct PSC or to exclude other conditions such as suspected overlap with autoimmune hepatitis.
- Antimitochondrial autoantibody testing can help exclude primary biliary cirrhosis.
- Patients with PSC should be tested at least once for elevated serum IgG4 levels.
- UDCA in doses >28 mg/kg/day should not be used for management of patients with PSC
- ERCP with balloon dilatation is recommended for PSC patients with dominant stricture and pruritus, and/or cholangitis, to relieve symptoms.
- PSC with a dominant stricture seen on imaging should have an ERCP with cytology, biopsies and FISH to exclude diagnosis of cholangiocarcinoma.
- PSC patients undergoing ERCP should have antibiotic prophylaxis to prevent post-ERCP cholangitis.
- Routine stenting after dilation of a dominant stricture is not required, whereas short-term stenting may be required in patients with severe stricture.
- Liver transplantation, when possible, is recommended over medical therapy or surgical drainage in PSC patients with decompensated cirrhosis, to prolong survival
- Patients should be referred for liver transplantation when their MELD score exceeds 14.
- Annual colon surveillance preferably with chromoendoscopy is recommended in PSC patients with colitis beginning at the time of PSC diagnosis.
- A full colonoscopy with biopsies is recommended in patients with PSC regardless of the presence of symptoms to assess for associated colitis at the time of PSC diagnosis.
- Some advocate repeating the exam every 3–5 years in those without prior evidence of colitis.
- Consider screening for cholangiocarcinoma with regular cross-sectional imaging with ultrasound or MR and serial CA 19-9 every 6–12 months.
- Cholecystectomy should be performed for patients with PSC and gallbladder polyps >8 mm, to prevent the development of gallbladder adenocarcinoma.
- Further testing for autoimmune hepatitis is recommended for patients <25 years of age with PSC or those with higher- than-expected levels of aminotransferases usually 5× upper limit of normal.
- MRCP is recommended for patients <25 years of age with autoimmune hepatitis, who have elevated serum ALP usually >2× the upper limit of normal.
- Local skin treatment should be performed with emollients and/or antihistamines in patients with PSC and mild pruritus, to reduce symptoms.
- Bile acid sequestrants such as cholestyramine should be taken (prescribed) in patients with PSC and moderate pruritus, to reduce symptoms. Second-line treatment such as rifampin and naltrexone can be considered if cholestyramine is ineffective or poorly tolerated.
- Recommend screening for varices in patients with signs of advanced disease with platelet counts <150×103/dl.
- Patients with PSC should undergo BMD screening at diagnosis with dual energy X-ray absorption at diagnosis and repeated at 2- to 4-year intervals.
- Patients with advanced liver disease should be screened and monitored for fat-soluble vitamin deficiencies.
Diagnosis and Management of Idiosyncratic Drug-Induced Liver Injury
Please review the ACG Clinical Guideline on The Diagnosis and Management of Idiosyncratic Drug-Induced Liver Injury
Idiosyncratic drug-induced liver injury (DILI) is a rare adverse drug reaction and it can lead to jaundice, liver failure, or even death. Antimicrobials and herbal and dietary supplements are among the most common therapeutic classes to cause DILI in the Western world. DILI is a diagnosis of exclusion and thus careful history taking and thorough work-up for competing etiologies are essential for its timely diagnosis. In this ACG Clinical Guideline, the authors present an evidence-based approach to diagnosis and management of DILI with special emphasis on DILI due to herbal and dietary supplements and DILI occurring in individuals with underlying liver disease. Download the Guideline for your review.
Terminology and definitions
Intrinsic DILI – Hepatotoxicity with potential to affect all individuals to varying degrees. Reaction typically stereotypic and dose dependent (e.g., acetaminophen).
Idiosyncratic DILI – Hepatotoxicity affecting only rare susceptible individuals. Reaction less dose dependent and more varied in latency, presentation, and course.
Chronic DILI – Failure of return of liver enzymes or bilirubin to pre-DILI baseline, and/or other signs or symptoms of ongoing liver disease (e.g., ascites, encephalopathy, portal hypertension, coagulopathy) 6 months after DILI onset.
Latency – Time from medication (or HDS) start to onset of DILI.
Wash-out, resolution, or de-challenge – Time from DILI onset to return of enzymes and/or bilirubin to pre-DILI baseline levels.
Rechallenge – Re-administration of medication or HDS to a patient who already had a DILI to the same agent.
Hy’s law – Observation made by late Hyman Zimmerman suggesting a 1 in 10 mortality risk of DILI if the following three criteria are met:
- Serum ALT or AST > 3 × ULN
- Serum total bilirubin elevated to > 2 × ULN, without initial findings of cholestasis (elevated serum alkaline phosphatase)
- No other reason can be found to explain the combination of increased aminotransferases and bilirubin, such as viral hepatitis A, B, C, or other preexisting or acute liver disease
Temple’s corollary – An imbalance in the frequency of ALT > 3 × ULN between active treatment and control arms in a randomized controlled trial. This is used to assess for hepatotoxic potential of a drug from premarketing clinical trials
R-value – ALT/ULN ÷ AP/ULN. Used to defined hepatotoxicity injury patterns: hepatocellular (R > 5), mixed (R =2 – 5), and cholestatic (R < 2)
RUCAM – Diagnostic algorithm that uses a scoring system based on clinical data, pre-existing hepatotoxicity literature on the suspected agent and rechallenge
Variables that may predispose individuals to idiosyncratic DILI
- Host factors
- Age
- Gender
- Pregnancy
- Malnutrition
- Obesity
- Diabetes mellitus
- Co-morbidities including underlying liver disease
- Indications for therapy
- Environmental factors
- Smoking
- Alcohol consumption
- Infection and inflammatory episodes
- Drug-related factors
- Daily dose
- Metabolic profile
- Class effect and cross-sensitization
- Drug interactions and polypharmacy
Recommended minimal elements of a diagnostic evaluation in the work-up of suspected DILI
- Gender – Particularly pertinent for competing disorders (e.g., PBC)
- Age – Particularly pertinent for competing disorders (e.g., HEV)
- Race/ethnicity – Particularly pertinent for competing disorders (e.g., sarcoidosis, sickle cell-related biliary stone disease, oriental sclerosing cholangitis)
- Indication for use of drug or herbal or dietary supplement (HDS)
- Concomitant diseases – Particularly pertinent disorders may include sepsis, heart failure, hypotension episodes, recent general anesthesia, parenteral nutrition, and cancer
- Presence of rechallenge – Give timing of rechallenge if done
- History of other drug reactions – Certain cross-reactivities may exist (e.g., anti-epileptics)
- History of other liver disorders – Chronic viral hepatitis, NAFLD, hemochromatosis, alcoholic liver disease, PSC, PBC, liver cancer
- History of alcohol use – Past vs. present; estimated grams per day; sporadic vs. binge drinking vs. regular (daily or weekly)
- Exposure time (“latency”) – Start and stop dates or total number of days, weeks, or months taken
- Symptoms and signs – Presence or absence, time of onset, type (fatigue, weakness, abdominal pain, nausea, dark urine, icterus, jaundice, pruritus, fever, rash)
- Physical findings – Fever, rash, hepatomegaly, hepatic tenderness, signs of chronic liver disease
- Medications and HDS products – Complete list of medications or HDS products with particular attention to those started in the previous 6 months
- Laboratory results – Day of first abnormal liver biochemistry; liver biochemistries, eosinophil counts at presentation
- Viral hepatitis serologies – Anti-HAV IgM, HBsAg, anti-HBc IgM, anti-HCV, HCV RNA
- Auto-immune hepatitis serologies – ANA, anti-smooth muscle antibody, IgG level
- Imaging – US± Doppler, CT, or MRI ± MRCP
- Histology, if available – Timing of biopsy in relation to enzyme elevation and onset
- Washout (de-challenge) data – Follow-up liver biochemistries
- Clinical outcome – Resolution, transplant, death, and timing of each
Most common or well-described DILI agents and the patterns of their liver injury
Agent – Latency – Typical pattern of injury/identifying features (short=3-30 days; moderate=30-90 days; long > 90 days).
- Antibiotics
- Amoxicillin/clavulanate – Short to moderate – Cholestatic injury, but can be hepatocellular; DILI onset is frequently detected after drug cessation
- Isoniazid – Moderate to long – Acute hepatocellular injury similar to acute viral hepatitis
- Trimethoprim/sulfamethoxazole – Short to moderate – Cholestatic injury, but can be hepatocellular; often with immunoallergic features (e.g., fever, rash, eosinophilia)
- Fluoroquinolones – Short – Variable: hepatocellular, cholestatic, or mixed in relatively similar proportions
- Macrolides – Short – Hepatocellular, but can be cholestatic
- Nitrofurantoin
- Acute form (rare) – Short – Hepatocellular
- Chronic form – Moderate to long (months – years) – Typically hepatocellular; often resembles idiopathic autoimmune hepatitis
- Minocycline – Moderate to long – Hepatocellular and often resembles autoimmune hepatitis
- Anti-epileptics
- Phenytoin – Short to moderate – Hepatocellular, mixed, or cholestatic often with immune-allergic features (e.g., fever, rash, eosinophilia) (anti-convulsant hypersensitivity syndrome)
- Carbamazepine – Moderate – Hepatocellular, mixed, or cholestatic often with immune-allergic features (anti-convulsant hypersensitivity syndrome)
- Lamotrigine – Moderate – Hepatocellular often with immune-allergic features (anti-convulsant hypersensitivity syndrome)
- Valproate
- Hyperammonemia – Moderate to long – Elevated blood ammonia, encephalopathy
- Hepatocellular – Moderate to long – Hepatocellular
- Reye-like syndrome – Moderate – Hepatocellular, acidosis; microvesicular steatosis on biopsy
- Analgesics
- Non-steroidal anti-inflammatory agents – Moderate to long – Hepatocellular injury
- Immune modulators
- Interferon-β – Moderate to long – Hepatocellular
- Interferon-α – Moderate – Hepatocellular, autoimmune hepatitis-like
- Anti-TNF agents – Moderate to long – Hepatocellular. Can have autoimmune hepatitis features
- Azathioprine – Moderate to long – Cholestatic or hepatocellular, but can present with portal hypertension (veno-occlusive disease, nodular regenerative hyperplasia)
- Herbals and dietary supplements
- Green tea extract (catechin) – Short to moderate – Hepatocellular
- Anabolic steroids – Moderate to long – Cholestatic; likely contained as adulterants in performance-enhancing products
- Pyrrolizidne alkaloids – Moderate to long – Sinusoidal obstruction syndrome / veno-occlusive disease; contained in some teas
- Flavocoxib – Short to moderate – Mixed hepatocellular and cholestatic
- Miscellaneous
- Methotrexate (oral) – Long – Fatty liver, fibrosis
- Allopurinol – Short to moderate – Hepatocellular or mixed. Often with immune-allergic features. Granulomas often present on biopsy
- Amiodarone (oral) – Moderate to long – Hepatocellular, mixed, or cholestatic. Macrovesicular steatosis and steatohepatitis on biopsy
- Androgen-containing steroids – Moderate to long – Cholestatic. Can present with peliosis hepatis, nodular regenerative hyperplasia, or hepatocellular carcinoma
- Inhaled anesthetics – Short – Hepatocellular. May have immune-allergic features ± fever
- Sulfasalazine – Short to moderate – Mixed, hepatocellular, or cholestatic. Often with immunoallergic features
- Proton pump inhibitors – Short – Hepatocellular; very rare
DILI: Summary statements and recommendations
- Accurate clinical history related to medication exposure and the onset of liver test abnormalities should be obtained when DILI is suspected.
- DILI is a diagnosis of exclusion, and thus appropriate competing etiologies should be excluded in a systematic manner.
- On the basis of the R-value at presentation, DILI can be categorized into hepatocellular, cholestatic, or mixed types. This categorization allows testing for competing etiologies in a systematic approach.
- Liver biopsy can help confirm a clinical suspicion of DILI, provide important information regarding disease severity, and also help exclude competing causes of liver injury.
- In individuals with suspected hepatocellular or mixed DILI:
- Acute viral hepatitis (A, B, and C) and autoimmune hepatitis should be excluded with standard serologies and HCV RNA testing.
- Routine anti-hepatitis E virus IgM testing cannot be recommended owing to unclear performance characteristics of the currently available commercial tests. However, it should be considered in the setting of heightened clinical suspicion (e.g., recent travel in an endemic area).
- Testing for acute cytomegalovirus, acute Epstein-Barr virus, or acute herpes simplex virus infection should be undertaken if classical viral hepatitis has been excluded or clinical features such as atypical lymphocytosis and lymphadenopathy suggest such causes.
- Wilson’s disease and Budd-Chiari syndrome should be considered when clinically appropriate
- In individuals with suspected cholestatic DILI:
- Abdominal imaging (ultrasound or computerized tomography scan) should be performed in all instances to exclude biliary tract pathology and infiltrative processes.
- Serological testing for primary biliary cirrhosis should be limited to those with no evidence of obvious biliary tract pathology on abdominal imaging.
- Endoscopic retrograde cholangiography should be limited to instances where routine imaging is unable to exclude impacted common bile duct stones, primary sclerosing cholangitis, or pancreatico-biliary malignancy.
- When to consider a liver biopsy?
- A liver biopsy should be considered if autoimmune hepatitis remains a competing etiology and if immunosuppressive therapy is contemplated.
- A liver biopsy may be considered in the following situations:
- If there is unrelenting rise in liver biochemistries or signs of worsening liver function despite stopping the suspected off ending agent,
- If the peak alanine aminotransferase level has not decreased by > 50 % at 30 – 60 days aft er the onset in cases of hepatocellular DILI, or if the peak alkaline phosphatase has not fallen by > 50 % at 180 days in cases of cholestatic DILI despite stopping the suspected off ending agent,
- In cases of DILI where continued use or re-exposure to the implicated agent is expected,
- If liver biochemistry abnormalities persist beyond 180 days to evaluate for the presence of chronic liver diseases (CLDs) and chronic DILI.
- In general, outcomes of idiosyncratic DILI are good, with only ~ 10 % reaching the threshold of ALF (coagulopathy and encephalopathy).
- DILI that does evolve to ALF carries a poor prognosis, with 40 % requiring liver transplantation and 42 % dying of the episode. Advanced coma grade and high MELD scores are associated with bad outcomes.
- Prognostic scores to predict outcome for DILI reaching the threshold of ALF are poor or rudimentary.
- Re-exposure to a drug that is thought likely to have caused hepatotoxicity is strongly discouraged, especially if the initial liver injury was associated with significant aminotransferase elevation (for example, > 5xULN, Hy ’ s law, or jaundice). An exception to this recommendation is in cases of life-threatening situations where there is no suitable alternative.
- In individuals with suspected DILI, especially when liver biochemistries are rising rapidly or there is evidence of liver dysfunction, the suspected agent(s) should be promptly stopped.
- No definitive therapies are available either for idiosyncratic DILI with or without ALF: however, NAC may be considered in adults with early-stage ALF, given its good safety profile and some evidence for efficacy in early coma stage patients.
- NAC is not recommended for children with severe DILI leading to ALF
Herbal or dietary supplement (HDS) induced liver injury
- HDS account for an increasing proportion of DILI events in the United States, with body building and weight loss supplements being the most commonly implicated.
- The current regulation for HDS differs substantially from conventional prescription medications. Most importantly, there is no requirement for premarketing safety analyses of HDS.
- Patients and providers must be aware that regulation is not rigorous enough to assure complete safety of marketed products. Patients should be made aware of this fact, and of the potential for HDS to cause liver injury.
- Current causality assessment approaches are not well suited for HDS hepatotoxicity, given the possibility of product variability and contamination; however, expert opinion is probably the best suited for HDS hepatotoxicity, as all information is taken into consideration in assigning a likelihood of injury.
- Voluntary reporting of suspected HDS hepatotoxicity cases through the FDA MEDWATCH system is essential.
- Patients should be encouraged to report the use of HDS to their health-care providers, and be reminded that supplements are not subjected to the same rigorous testing for safety and efficacy as are prescription medications.
- The same diagnostic approach for DILI is applicable to suspected HDS hepatotoxicity. That is, other forms of liver injury must be excluded through a careful history and appropriate laboratory testing and hepatobiliary imaging. Excluding other causes, the diagnosis of HDS hepatotoxicity can be made with confidence in the setting of recent use of HDS.
- Patients with suspected HDS hepatotoxicity should stop all HDS hepatotoxicity and be monitored for resolution of their liver injury.
DILI in patients with chronic liver disease (CLD)
- There are no data to show that underlying CLD is a major risk factor for all-cause DILI, but it may increase the risk for DILI due to selected medications. Patients with chronic HBV and HCV may be more prone to develop liver injury due to specific agents such as isoniazid and antiretrovirals, and may experience more severe outcomes.
- Individuals with underlying fatty liver disease are not at an increased risk for hepatotoxicity from statins.
- The diagnosis of DILI in patients with CLD requires a high index of suspicion and exclusion of other more common causes of acute liver injury, including a flare-up of the underlying liver disease.
- The use of potentially hepatotoxic drugs in CLD patients should be based upon the risk versus benefit of the proposed therapy on a case-by-case basis.
- There are no data to recommend a specific liver biochemistry monitoring plan when a potential hepatotoxic agent is prescribed in individuals with known CLD. Often, information contained in the package inserts is incomplete or unhelpful. Patients should be advised to promptly report any new-onset symptoms such as scleral icterus, abdominal pain / discomfort, nausea / vomiting, pruritis, or choluria. In addition, it is reasonable to monitor serum liver biochemistries at 4 – 6 week intervals, especially during the initial 6 months of treatment with a potentially hepatotoxic agent.
In Summary
- In individuals with suspected hepatocellular or mixed DILI:
- Acute viral hepatitis (A, B, and C) and auto-immune hepatitis should be excluded with standard serologies and HCV RNA testing.
- Anti-HEV IgM testing cannot be recommended because of unclear performance characteristics of the currently available commercial tests. However, it should be considered in the setting of heightened clinical suspicion (e.g., recent travel in an endemic area).
- Testing for acute CMV, acute EBV, or acute HSV infection should be undertaken if classical viral hepatitis has been excluded or clinical features such as atypical lymphocytosis, lymphadenopathy suggest such causes.
- Wilson’s disease and Budd-Chiari syndrome should be considered when clinically appropriate.
- In individuals with suspected cholestatic DILI:
- Abdominal imaging (ultrasound or CT scan) should be performed in all instances to exclude biliary tract pathology and infi ltrative processes.
- Serological testing for primary biliary cirrhosis should be limited to those with no evidence of obvious biliary tract pathology on abdominal imaging.
- Endoscopic retrograde cholangiography should be limited to instances where routine imaging is unable to exclude impacted common bile duct stones, primary sclerosing cholangitis, or pancreatico-biliary malignancy.
- When to consider a liver biopsy?
- A liver biopsy should be considered if autoimmune hepatitis remains a competing etiology and if immunosuppressive therapy is contemplated.
- A liver biopsy may be considered:
- If there is unrelenting rise in liver biochemistries or signs of worsening liver function despite stopping the suspected offending agent.
- If peak ALT level has not fallen by > 50 % at 30 – 60 days after onset in cases of hepatocellular DILI, or if peak Alk P has not fallen by > 50 % at 180 days in cases of cholestatic DILI despite stopping the suspected offending agent.
- In cases of DILI where continued use or re-exposure to the implicated agent is expected.
- If liver biochemistry abnormalities persist beyond 180 days to evaluate for the presence of chronic liver diseases and chronic DILI.
- Re-exposure to a drug thought likely to have caused hepatotoxicity is strongly discouraged, especially if the initial liver injury was associated with significant aminotransferase elevation (e.g., > 5xULN, Hy’s law), or jaundice. An exception to this recommendation is in cases of life-threatening situations where there is no suitable alternative.
- In individuals with suspected DILI, especially when liver biochemistries are rising rapidly or there is evidence of liver dysfunction, suspected agent(s) should be promptly stopped.
- No definitive therapies are available either for idiosyncratic DILI with or without ALF: however, NAC may be considered in adults with early-stage ALF, given its good safety profile and some evidence for efficacy in early coma stage patients.
- NAC is not recommended for children with severe DILI leading to ALF.
- Patients should be encouraged to report use of HDS to their health-care providers, and be reminded that supplements are not subjected to the same rigorous testing for safety and efficacy as are prescription medications.
- The same diagnostic approach for DILI is applicable to suspected HDS-hepatotoxicity. That is, other forms of liver injury must be excluded through a careful history, and appropriate laboratory testing and hepatobiliary imaging. Excluding other causes, the diagnosis of HDS-hepatotoxicity can be made with confidence in the setting of recent use of HDS.
- Patients with suspected HDS-hepatotoxicity should stop all HDS-hepatotoxicity and be monitored for resolution of their liver injury.
- The diagnosis of DILI in patients with CLD requires a high index of suspicion and exclusion of other more common causes of acute liver injury including a flare-up of the underlying liver disease.
- The use of potentially hepatotoxic drugs in CLD patients should be based upon the risk vs. benefit of the proposed therapy on a case-by-case basis.
- There are no data to recommend a specific liver biochemistry monitoring plan when a potential hepatotoxic agent is prescribed in individuals with known CLD. Often, information contained in the package inserts is incomplete or unhelpful. Patients should be advised to promptly report any new onset symptoms such as yellowing of their eyes, abdominal pain / discomfort, nausea / vomiting, itching, or dark urine. In addition, it is reasonable to monitor serum liver biochemistries at 4 – 6 weekly intervals, especially during the initial 6 months of treatment with a potentially hepatotoxic agent.
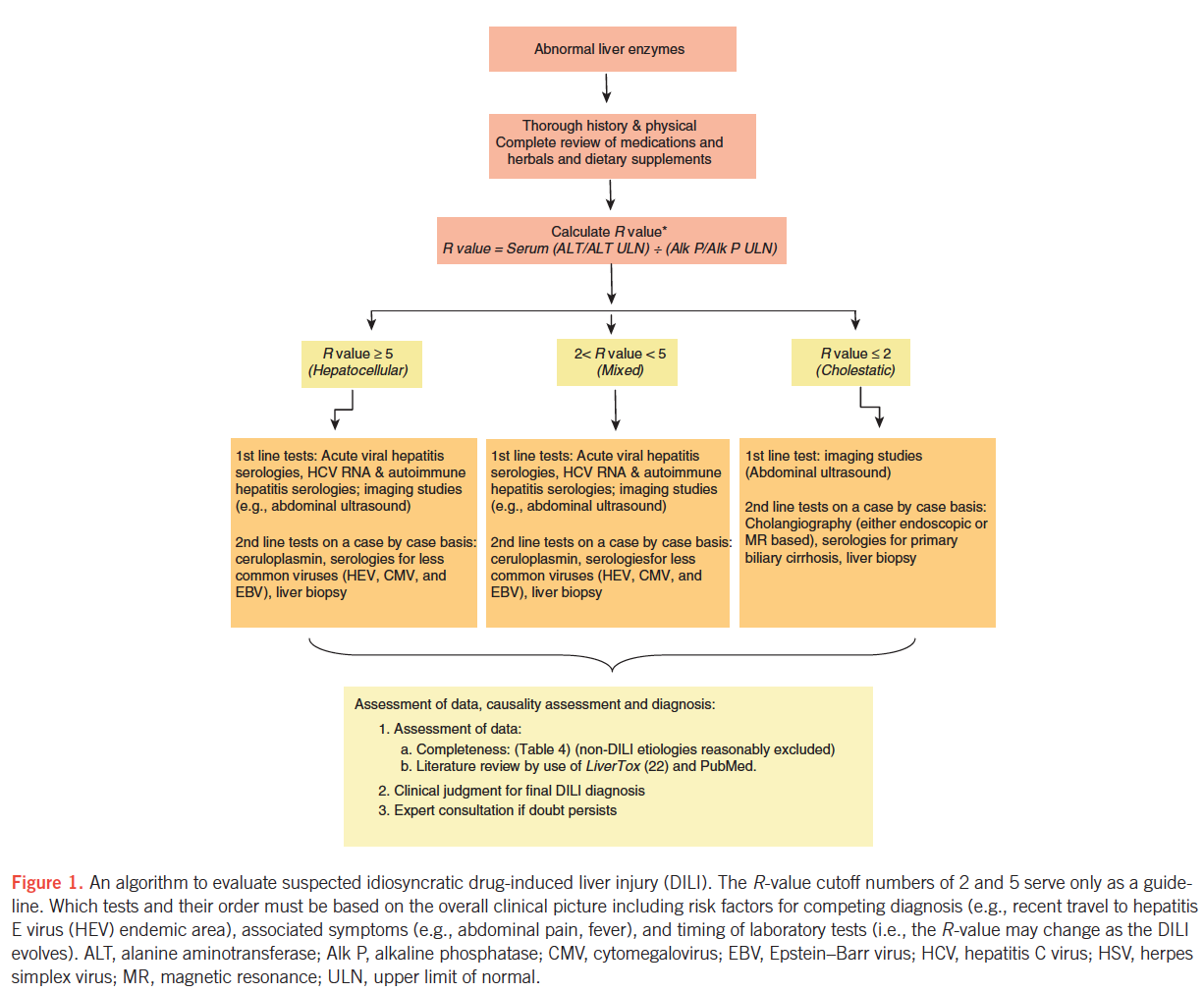
Am J Gastroenterol advance online publication, 17 June 2014; doi: 10.1038/ajg.2014.131
Abbreviations:
ALF, acute liver failure;
Alk P, alkaline phosphatase;
ALT, alanine aminotransferase;
ANA, anti-nuclear antibody;
AP, alkaline phosphatase;
AST, aspartate aminotransferase;
CLD, chronic liver disease
CMV, cytomegalovirus;
CT, computerized tomography;
DILI, drug-induced liver injury;
EBV, Epstein-Barr virus;
HAV, hepatitis A virus;
HBc, hepatitis B core antigen;
HBs, hepatitis B surface antigen;
HCV, hepatitis C virus;
HDS, herbal or dietary supplement;
HEV, hepatitis E virus;
HSV, herpes simplex virus;
NAC, N-acetyl cysteine:
NAFLD, nonalcoholic fatty liver disease;
PBC, primary biliary cirrhosis;
PSC, primary sclerosing cholangitis;
Ig, immunoglobulin;
MRI, magnetic resonance imaging;
MRCP, magnetic resonance cholangiopancreatography;
RUCAM, Roussel Uclaf Causality Assessment Method;
TNF, tumor necrosis factor;
ULN, upper limit of normal.
US, ultrasound.
