Home » Liver
Category Archives: Liver
AASLD Guidelines for Treatment of Chronic Hepatitis B
The American Association for the Study of Liver Diseases (AASLD) has released comprehensive guidelines for the treatment of chronic hepatitis B (CHB).
CHB affects more than 240 million people globally, causing significant morbidity and mortality. This document focuses on using antiviral therapy in chronic HBV infection and does not address other related and important issues, such as screening, prevention, and surveillance. For broader issues related to diagnosis, surveillance, and prevention as well as treatment in special populations (e.g., liver transplant recipients) that are not addressed by this guideline, the previous AASLD guideline and recent World Health Organization (WHO) guideline are excellent additional resources.
The AASLD formulated a list of discrete questions that physicians are faced with in daily practice.
These questions were:
- Should adults with immune active CHB be treated with antiviral therapy to decrease liver-related complications?
- Should adults with immune-tolerant infection be treated with antiviral therapy to decrease liver-related complications?
- Should antiviral therapy be discontinued in hepatitis B e antigen (HBeAg)-positive persons who have developed HBeAg seroconversion on therapy?
- Should antiviral therapy be discontinued in persons with HBeAg-negative infection with sustained HBV DNA suppression on therapy?
In HBV-monoinfected persons, does entecavir therapy, when compared to tenofovir therapy, have a different impact on renal and bone health? - Is there a benefit to adding a second antiviral agent in persons with persistent low levels of viremia while being treated with either tenofovir or entecavir?
- Should persons with compensated cirrhosis and low levels of viremia be treated with antiviral agents?
- Should pregnant women who are hepatitis B surface antigen (HBsAg) positive with high viral load receive antiviral treatment in the third trimester to prevent perinatal transmission of HBV?
- Should children with HBeAg-positive CHB be treated with antiviral therapy to decrease liver-related complications?
Natural History in Adults and Children
CHB has been traditionally characterized into four phases, reflecting the dynamic relationship between viral replication and evolution and the host immune response. These phases are of variable duration and not every person infected with CHB will evolve through all phases. Given the dynamic nature of CHB infection, serial monitoring of HBV DNA and alanine aminotransferase (ALT) levels is important to characterize the phase of infection. A single ALT and HBV DNA level are insufficient to assign phase of infection and/or need for treatment. Of note, some persons will be in the “gray zones,” meaning that their HBV DNA and ALT levels do not fall into the same phase. Longitudinal follow-up of ALT and HBV DNA levels and/or assessment of liver histology can serve to clarify the phase of infection.
- Immune-tolerant phase: In this highly replicative/low inflammatory phase, HBV DNA levels are elevated, ALT levels are normal (<19 U/L for females and <30 U/L for males), and biopsies are without signs of significant inflammation or fibrosis. The duration of this phase is highly variable, but longest in those who are infected perinatally. With increasing age, there is an increased likelihood of transitioning from immune-tolerant to the HBeAg-positive immune-active phase.
- HBeAg-positive immune-active phase: Elevated ALT and HBV DNA levels in conjunction with liver injury characterize this phase. Median age of onset is 30 years among those infected at a young age. The hallmark of transition from the HBeAg-positive immune-active to -inactive phases is HBeAg seroconversion. The rate of spontaneous seroconversion from HBeAg to antibody to HBeAg (anti-HBe) is less than 2% per year in children younger than 3 years of age and increases during puberty and among adults to 8% and 12% per year, respectively.
- Inactive CHB phase: In this phase, HBV DNA levels are low or undetectable, ALT levels are normal, and anti-HBe is present. Liver histology shows minimal necroinflammation, but variable fibrosis reflecting previous liver injury during the HBeAg-positive immune-active phase. Among persons who undergo spontaneous HBeAg seroconversion, 67%-80% will continue to remain in the inactive CHB phase. Approximately 4%-20% of inactive carriers have one or more reversions back to HBeAg positive.
- HBeAg-negative immune reactivation phase: Among those who seroconvert from HBeAg to anti-HBe positive, 10%-30% continue to have elevated ALT and high HBV DNA levels, and roughly 10%-20% of inactive carriers may have reactivation of HBV replication and exacerbations of hepatitis after years of quiescence. Most of these persons harbor HBV variants in the precore or core promoter region, and liver histology shows necroinflammation and fibrosis. Persons with HBeAg-negative CHB tend to have lower serum HBV DNA levels than those with HBeAg-positive CHB and are more likely to experience a fluctuating course.
The risk of liver-related complications is variable. Among untreated adults with CHB, the cumulative 5-year incidence of cirrhosis is 8%-20%, and among those with cirrhosis, 5-year cumulative risk of hepatic decompensation is 20%, and risk of HCC is 2%-5%. Viral, host, and environmental factors influence risks of cirrhosis and HCC. HBV DNA levels, ALT levels, and HBeAg status are among the most important determinants of risk of progression to cirrhosis, whereas HBV DNA levels (>2,000 IU/mL), HBeAg status, and cirrhosis are key predictors of HCC risk. A biological gradient of risk has been shown in adults with HBV DNA levels above 2,000 IU/mL; a higher HBV DNA level is associated with progressively higher rates of cirrhosis and HCC.
The initial evaluation of persons with CHB should include
- a thorough history and physical examination
- emphasis on risk factors for coinfection, alcohol use, and family history of HBV infection and liver cancer
- Laboratory tests should include
- assessment of liver disease activity and function
- markers of HBV replication
- tests for coinfection with
- hepatitis C virus (HCV)
- hepatitis delta virus (HDV)
- human immunodeficiency virus (HIV) in those at risk.
Owing to the fluctuating nature of CHB, the accuracy of one high HBV DNA level at a single time point in predicting prognosis is poor and regular monitoring of disease status is imperative to determine need for antiviral therapy. The upper limits of normal (ULNs) for ALT values based on healthy subjects are lower than laboratory values derived from all populations, including those with subclinical liver disease.
Determination of the stage of liver disease is important in guiding antiviral therapy decisions and need for surveillance.
- Liver biopsy provides an assessment of the severity of necroinflammation and fibrosis, rules out other causes of liver disease, and may be especially useful for persons who lack clear-cut indications for treatment. Liver biopsy is regarded as the best method to assess the severity of inflammatory activity and fibrosis,
- Noninvasive methods to assess fibrosis severity are also useful, but:
- Acute-on-chronic exacerbations of hepatitis B may lead to overestimation of fibrosis stage by noninvasive tests, and different cutoffs for significant and advanced fibrosis depending on ALT levels have been proposed.
- Serum markers of fibrosis, such as aspartate aminotransferase (AST)-to-platelet ratio index (APRI), FIB-4, FibroTest, and vibration-controlled transient elastography, have only moderate accuracy in identifying persons with significant fibrosis (fibrosis stage 2 or greater on the Metavir scale), but good diagnostic accuracy in excluding advanced fibrosis and may be useful aids in decision making.
Antiviral Therapy
The goals of antiviral treatment are to decrease the morbidity and mortality related to CHB. The achievement of a sustained suppression of HBV replication has been associated with normalization of serum ALT, loss of HBeAg with or without detection of (anti-HBe), and improvement in liver histology. Historically, the term “cure” was avoided in treatment of CHB, given that persistence of covalently closed circular DNA (cccDNA) in the nucleus of hepatocytes, even in persons with serological markers of resolved infection, poses a lifelong risk for reactivation of infection. However, an immunological cure may be defined by HBsAg loss and sustained HBV DNA suppression and a virological cure defined by eradication of virus, including the cccDNA form. The latter is not currently an attainable goal.
There are six therapeutic agents approved for the treatment of adults with CHB in the United States and five therapeutic agents approved for the treatment of children with CHB. Side effects are more frequent with interferon (IFN) therapy than with nucleos(t)ide analogs (NAs) therapy. Overall, all NAs have an excellent safety profile across a wide spectrum of persons with CHB, including those with decompensated cirrhosis and transplant recipients. For persons with HDV coinfection, the only effective treatment is pegylated interferon (Peg-IFN). For persons with HIV coinfection, treatment of HBV needs to be coordinated with HIV therapy given that several HBV drugs have anti-HIV activity (tenofovir, entecavir, lamivudine, and telbivudine).
The guideline answers the above stated critical questions:
- Should adults with immune active CHB be treated with antiviral therapy to decrease liver-related complications?
- Treatment Intervention: Antiviral therapy
Comparison: No treatment
Outcome: Cirrhosis, decompensation, HCC, death, loss of HBsAg - Recommendations: The AASLD recommends antiviral therapy for adults with immune-active CHB (HBeAg negative or HBeAg positive) to decrease the risk of liver-related complications. The AASLD also recommends Peg-IFN, entecavir, or tenofovir as preferred initial therapy for adults with immune-active CHB.
- Treatment Intervention: Antiviral therapy
- Should adults with immune-tolerant infection be treated with antiviral therapy to decrease liver-related complications?
- Treatment Intervention: Antiviral therapy
Comparison: No treatment
Outcome: Cirrhosis, decompensation, HCC, death, loss of HBsAg - Recommendations: The AASLD recommends against antiviral therapy for adults with immune-tolerant CHB. The AASLD suggests that ALT levels be tested at least every 6 months for adults with immune-tolerant CHB to monitor for potential transition to immune-active or -inactive CHB. The AASLD suggests antiviral therapy in the select group of adults >40 years of age with normal ALT and elevated HBV DNA (≥1,000,000 IU/mL) and liver biopsy showing significant necroinflammation or fibrosis.
- Treatment Intervention: Antiviral therapy
- Should antiviral therapy be discontinued in hepatitis B e antigen (HBeAg)-positive persons who have developed HBeAg seroconversion on therapy?
- Treatment Intervention: Continued antiviral therapy
Comparison: Stopping antiviral therapy
Outcome: Cirrhosis, HCC, reactivation, seroreversion, decompensation, loss of HBsAg - Recommendations: The AASLD suggests that HBeAg-positive adults without cirrhosis with CHB who seroconvert to anti-HBe on therapy discontinue NAs after a period of treatment consolidation. The AASLD suggests indefinite antiviral therapy for HBeAg-positive adults with cirrhosis with CHB who seroconvert to anti-HBe on NA therapy, based on concerns for potential clinical decompensation and death, unless there is a strong competing rationale for treatment discontinuation.
- Treatment Intervention: Continued antiviral therapy
- Should antiviral therapy be discontinued in persons with HBeAg-negative infection with sustained HBV DNA suppression on therapy?
- Treatment Intervention: Continued antiviral therapy
Comparison: Stopping antiviral therapy
Outcome: Reactivation, decompensation, loss of HBsAg - Recommendations: The AASLD suggests indefinite antiviral therapy for adults with HBeAg-negative immune-active CHB, unless there is a competing rationale for treatment discontinuation.
- Treatment Intervention: Continued antiviral therapy
- In HBV-monoinfected persons, does entecavir therapy, when compared to tenofovir therapy, have a different impact on renal and bone health?
- Treatment Intervention: Tenofovir
Comparison: Entecavir
Outcome: Renal function, hypophosphatemia, bone health - Recommendations: The AASLD suggests no preference between entecavir and tenofovir regarding potential long-term risks of renal and bone complications.
- Treatment Intervention: Tenofovir
- Is there a benefit to adding a second antiviral agent in persons with persistent low levels of viremia while being treated with either tenofovir or entecavir?
- Treatment Intervention: Continue therapy
Comparison: Change or switch therapy
Outcome: HBV resistance, clinical flare, decompensation, loss of HBeAg - Recommendations: The AASLD suggests that persons with persistent low-level viremia (<2,000 IU/mL) on entecavir or tenofovir monotherapy continue monotherapy, regardless of ALT. The AASLD suggests one of two strategies in persons with virological breakthrough on entecavir or tenofovir monotherapy: either switch to another antiviral monotherapy with high barrier to resistance or add a second antiviral drug that lacks cross-resistance.
- Treatment Intervention: Continue therapy
- Should persons with compensated cirrhosis and low levels of viremia be treated with antiviral agents?
- Treatment Intervention: Antiviral therapy
Comparison: No treatment
Outcome: Decompensation, HCC, death - Recommendations: The AASLD suggests that adults with compensated cirrhosis and low levels of viremia (<2,000 IU/mL) be treated with antiviral therapy to reduce the risk of decompensation, regardless of ALT level. The AASLD recommends that HBsAg-positive adults with decompensated cirrhosis be treated with antiviral therapy indefinitely regardless of HBV DNA level, HBeAg status, or ALT level to decrease risk of worsening liver-related complications.
- Treatment Intervention: Antiviral therapy
- Should pregnant women who are hepatitis B surface antigen (HBsAg) positive with high viral load receive antiviral treatment in the third trimester to prevent perinatal transmission of HBV?
- Treatment Intervention: Antiviral therapy in third trimester
Comparison: No treatment
Outcome: Cirrhosis, decompensation, HCC, death, loss of HBsAg CHB in the infant, maternal safety, fetal/infant safety - Recommendations: The AASLD suggests antiviral therapy to reduce the risk of perinatal transmission of hepatitis B in HBsAg-positive pregnant women with an HBV DNA level >200,000 IU/mL. The AASLD recommends against the use of antiviral therapy to reduce the risk of perinatal transmission of hepatitis B in the HBsAg-positive pregnant woman with an HBV DNA ≤200,000 IU/mL.
- Treatment Intervention: Antiviral therapy in third trimester
- Should children with HBeAg-positive CHB be treated with antiviral therapy to decrease liver-related complications?
- Treatment Intervention: Antiviral therapy
Comparison: No treatment
Outcome: Cirrhosis, decompensation, HCC, death, HBeAg seroconversion, loss of HBsAg - Recommendations: The AASLD suggests antiviral therapy in HBeAg-positive children (ages 2 to <18 years) with both elevated ALT and measurable HBV DNA levels, with the goal of achieving sustained HBeAg seroconversion. The AASLD recommends against use of antiviral therapy in HBeAg-positive children (ages 2 to <18 years) with persistently normal ALT, regardless of HBV DNA level.
- Treatment Intervention: Antiviral therapy
Summary of Recommendations
- The AASLD recommends antiviral therapy for adults with immune-active CHB (HBeAg negative or HBeAg positive) to decrease the risk of liver-related complications.
- The AASLD recommends Peg-IFN, entecavir, or tenofovir as preferred initial therapy for adults with immune-active CHB.
- The AASLD recommends against antiviral therapy for adults with immune-tolerant CHB.
- The AASLD suggests that ALT levels be tested at least every 6 months for adults with immune-tolerant CHB to monitor for potential transition to immune-active or -inactive CHB.
- The AASLD suggests antiviral therapy in the select group of adults >40 years of age with normal ALT and elevated HBV DNA (≥1,000,000 IU/mL) and liver biopsy showing significant necroinflammation or fibrosis.
- The AASLD suggests that HBeAg-positive adults without cirrhosis with CHB who seroconvert to anti-HBe on therapy discontinue NAs after a period of treatment consolidation.
- The AASLD suggests indefinite antiviral therapy for HBeAg-positive adults with cirrhosis with CHB who seroconvert to anti-HBe on NA therapy, based on concerns for potential clinical decompensation and death, unless there is a strong competing rationale for treatment discontinuation.
- The AASLD suggests indefinite antiviral therapy for adults with HBeAg-negative immune-active CHB, unless there is a competing rationale for treatment discontinuation.
- The AASLD suggests no preference between entecavir and tenofovir regarding potential long-term risks of renal and bone complications.
- The AASLD suggests that persons with persistent low-level viremia (<2,000 IU/mL) on entecavir or tenofovir monotherapy continue monotherapy, regardless of ALT.
- The AASLD suggests one of two strategies in persons with virological breakthrough on entecavir or tenofovir monotherapy: either switch to another antiviral monotherapy with high barrier to resistance or add a second antiviral drug that lacks cross-resistance.
- The AASLD suggests that adults with compensated cirrhosis and low levels of viremia (<2,000 IU/mL) be treated with antiviral therapy to reduce the risk of decompensation, regardless of ALT level.
- The AASLD recommends that HBsAg-positive adults with decompensated cirrhosis be treated with antiviral therapy indefinitely regardless of HBV DNA level, HBeAg status, or ALT level to decrease risk of worsening liver-related complications.
- The AASLD suggests antiviral therapy to reduce the risk of perinatal transmission of hepatitis B in HBsAg-positive pregnant women with an HBV DNA level >200,000 IU/mL.
- The AASLD recommends against the use of antiviral therapy to reduce the risk of perinatal transmission of hepatitis B in the HBsAg-positive pregnant woman with an HBV DNA ≤200,000 IU/mL.
- The AASLD suggests antiviral therapy in HBeAg-positive children (ages 2 to <18 years) with both elevated ALT and measurable HBV DNA levels, with the goal of achieving sustained HBeAg seroconversion.
- The AASLD recommends against use of antiviral therapy in HBeAg-positive children (ages 2 to <18 years) with persistently normal ALT, regardless of HBV DNA level.
Abbreviations
ALT alanine aminotransferase
anti-HBe antibody to HBeAg
anti-HBs antibody to HBsAg
APRI AST-to-platelet ratio index
AST aspartate aminotransferase
cccDNA covalently closed circular DNA
CHB chronic hepatitis B
HBV hepatitis B virus
HCV hepatitis C virus
HCC hepatocellular carcinoma
HIV human immunodeficiency virus
HDV hepatitis delta virus
HBsAg hepatitis B surface antigen
HBeAg hepatitis B e antigen
IFN interferon
NA nucleos(t)ide analog
Peg-IFN pegylated interferon
http://www.aasld.org/sites/default/files/guideline_documents/hep28156.pdf
http://onlinelibrary.wiley.com/doi/10.1002/hep.28156/full
ACG Clinical Guideline: Primary Sclerosing Cholangitis
- Differential diagnosis of primary sclerosing cholangitis
- Secondary sclerosing cholangitis
- Cholangiocarcinoma
- IgG4-associated cholangitis
- Histiocytosis X
- Autoimmune hepatitis
- HIV syndrome
- Bile duct strictures
- Cholendocholithiasis
- Primary biliary cirrhosis
- Papillary tumors
- Diagnosis
- Endoscopic retrograde cholangiopancreatography (ERCP) has been the most common procedure in diagnosing PBS. However, magnetic resonance cholangiopancreatography (MRCP) is rapidly becoming the preferred method because it is noninvasive, cheaper and has no associated risk of pancreatitis. A liver biopsy is not needed unless a patient is suspected of having small duct PSC.
- Therapy
- There is currently no established treatment for PSC. However, clinicians are using doses of ursodeoxycholic acid at 20 mg/kg per day for treating PSC.
- Endoscopic Management
- Endoscopic treatment of dominant strictures may improve prognosis, help to relieve the complications of pruritus and cholangitis, allow for early diagnosis of cholangiocarcinoma and may lead to improved survival. ERCP with balloon dilatation is recommended for relieving symptoms of dominant strictures of PSC patients. If a PSC patient undergoes ERCP, antibiotic prophylaxis should be taken to prevent post-ERCP cholangitis. Routine stenting after dilation is not recommended.
- IBD and PSC
- Up to 80% of patients with PSC have IBD. Undergoing annual colon surveillance is recommended in PSC patients with colitis at the time of PCS diagnosis. A colonoscopy with biopsies is recommended in PSC patients whether or not there are symptoms at PSC diagnosis. An exam every 3-5 years is also recommended for patients without prior evidence of colitis.
- Hepatobiliary Malignancies and Gallbladder Disease
- PSC patients are at risk for developing hepatobiliary malignancies. The risk for cholangiocarcinoma is several hundred times higher in patients with PSC vs. patients without PSC. Screening for cholangiocarcinoma with regular cross-sectional imaging with ultrasound or magnetic resonance and serial CA 19-9 is recommended every 6 to 12 months. Patients with PSC with gallbladder polyps more than 8 mm should also undergo cholecystectomy.
- Special Situations
- Every PSC patient is unique and some patients may develop autoimmune hepatitis and other infections. Testing for autoimmune hepatitis is recommended for patients with PSC under 25 years of age and for those patients with higher than expected aminotransferases. MRCP is recommended for PSC patients under 25 years of age with autoimmune hepatitis who have elevated alkaline phosphatase serum levels.
- General Management
- Patients with PSC should undergo bone mineral density screening at diagnosis using duel energy X-ray absorption repeated at 2- to 4-year intervals; patients with advanced liver disease should be checked and monitored for fat-soluble vitamin deficiencies; and patients with PSC and mild pruritus should undergo local skin treatment with antihistamines or emollients to reduce symptoms.
- MRCP is preferred over endoscopic retrograde cholangiopancreatography (ERCP) to establish a diagnosis of PSC.
- Liver biopsy is not necessary to make a diagnosis in patients with suspected PSC based on diagnostic cholangiographic findings.
- Liver biopsy is recommended to make a diagnosis in patients with suspected small duct PSC or to exclude other conditions such as suspected overlap with autoimmune hepatitis.
- Antimitochondrial autoantibody testing can help exclude primary biliary cirrhosis.
- Patients with PSC should be tested at least once for elevated serum immunogloblulin G4 (IgG4) levels.
- At this time, there is no established medical treatment for patients with PSC.
- Ursodeoxycholic acid (UDCA) in doses >28 mg/kg/day should not be used for the management of patients with PSC.
- Other treatments that have been tested without any obvious proven clinical benefit or improvement of liver biochemistries include:
- Azathioprine
- Budesonide
- Docosahexaenoic acid
- Methotrexate
- Metronidazole
- Minocycline
- Mycophenolate mofetil
- Nicotine
- Pentoxifylline
- Pirfenodone
- Prednisolone
- Tacrolimus
- Vancomycin
- ERCP with balloon dilatation is recommended for PSC patients with dominant stricture and pruritus, and/or cholangitis, to relieve symptoms.
- PSC with a dominant stricture seen on imaging should have an ERCP with cytology, biopsies, and fluorescence in-situ hybridization (FISH), to exclude diagnosis of cholangiocarcinoma.
- PSC patients undergoing ERCP should have antibiotic prophylaxis to prevent post-ERCP cholangitis.
- Routine stenting after dilation of a dominant stricture is not required, whereas short-term stenting may be required in patients with severe stricture.
- Percutaneous cholangiography for treatment of dominant strictures can be performed in PSC patients with altered anatomy that prevents successful ERCP, such as Roux-en-Y choledo-chojejunostomy or gastric bypass, or as a rescue therapy after failed endoscopic access. Percutaneous cholangiography is generally the second line of treatment after ERCP because of the risk of complications, including hepatic arterial injury, hemobilia, and cholangitis
- Liver transplantation, when possible, is recommended over medical therapy or surgical drainage in PSC patients with decompensated cirrhosis, to prolong survival.
- Patients should be referred for liver transplantation when their Model for End-Stage Liver Disease (MELD) score exceeds 14.
- In specific clinical circumstances, patients with PSC may be offered additional MELD points, to improve their priority for receiving a donor organ for liver transplantation. MELD exception points can be approved by the United Network for Organ Sharing Regional Review Board for the following indications:
- Recurrent episodes of cholangitis, with >2 episodes of bacteremia or >1 episode of sepsis.
- Cholangiocarcinoma less then 3 cm in diameter, without evidence of metastasis, undergoing treatment through an institutional review board-approved clinical trial.
- Intractable pruritus.
- Recurrence of PSC after liver transplantation is relatively common, affecting as many as 20% of patients at 5 years after transplantation.
- The risk of colorectal dysplasia and cancer is significantly higher (approximately four- to fivefold) among patients with PSC and IBD compared with those with IBD without PSC.
- Annual colon surveillance preferably with chromoendoscopy is recommended in PSC patients with colitis beginning at the time of PSC diagnosis.
- A full colonoscopy with biopsies is recommended in patients with PSC regardless of the presence of symptoms to assess for associated colitis at time of PSC diagnosis.
- Some advocate repeating the exam every 3–5 years in those without prior evidence of colitis.
- Consider screening for cholangiocarcinoma with regular cross-sectional imaging with ultrasound or MR and serial CA 19-9 every 6–12 months.
- Cholecystectomy should be performed for patients with PSC and gallbladder polyps >8 mm, to prevent the development of gallbladder adenocarcinoma.
- PSC and autoimmune hepatitis may co-exist in the same patient and the prevalence of autoimmune hepatitis in patients with PSC is ~10%.
- Further testing for autoimmune hepatitis is recommended for patients with PSC <25 years of age or those with higher- than-expected levels of aminotransferases usually 5× upper limit of normal.
- MRCP is recommended for patients <25 years of age with autoimmune hepatitis, who have elevated serum ALP usually greater than 2× the upper limit of normal.
- PSC appears to be much less common among children than adults, with an estimated prevalence 20% lower than in adults and is a rare indication for liver transplantation in this population. PSC in children is more often associated with higher serum aminotransferase levels and concomitant autommune hepatitis, and sclerosing cholangitis is a more common phenomenon, leading to the use of the term “autoimmune sclerosing cholangitis.” Serum ALP may be elevated in children due to bone growth; hence, suspected cholestasis should be confirmed by measurement of gamma-glutamyl transpeptidase levels. Cholangiocarcinoma appears to be rare in this population and surveillance for gallbladder cancer or cholangiocarcinoma is not recommended.
- IgG4-associated pancreatitis and cholangitis is being increasingly recognized in patients who present with sclerosing cholangitis. IgG4-associated autoimmune pancreatitis is a clearly described entity characterized by strictures in the pancreatic duct, elevated IgG4 levels and response to immunosuppressive therapy. This condition may be associated with biliary strictures and elevated plasma IgG4 levels, and liver biopsy may reveal a lymphoplasmacytic infiltrate . In some cases, the biliary disease is predominant and features of autoimmune pancreatitis may or may not be present.
- Measurement of IgG4 levels is reasonable in patients with PSC and consideration should be given to imaging for autoimmune pancreatitis and the presence of IgG4-associated cholangitis among those with markedly elevated IgG4 levels.
- Liver biopsy should be considered to identify the classical lymphoplasmacytic infiltrate and consideration of immunosuppression therapy may be useful in such patients, especially if they have higher-than- expected elevations of serum aminotransferase levels.
- Local skin treatment should be performed with emollients and/or antihistamines in patients with PSC and mild pruritus, to reduce symptoms.
- Bile acid sequestrants such as cholestyramine should be taken (prescribed) in patients with PSC and moderate pruritus to reduce symptoms. Second-line treatment such as rifampin and naltrexone can be considered if cholestyramine is ineffective or poorly tolerated.
- Recommend screening for varices in patients with signs of advanced disease with platelet counts <150×103/dl.
- Patients with PSC should undergo bone mineral density (BMD) screening at diagnosis with dual energy X-ray absorption at diagnosis and repeated at 2- to 4-year intervals.
- Patients with advanced liver disease should be screened and monitored for fat-soluble vitamin deficiencies.
- MRCP is preferred over ERCP to establish a diagnosis of PSC.
- Liver biopsy is not necessary to make a diagnosis in patients with suspected PSC based on diagnostic cholangiographics findings.
- Liver biopsy is recommended to make a diagnosis in patients with suspected small duct PSC or to exclude other conditions such as suspected overlap with autoimmune hepatitis.
- Antimitochondrial autoantibody testing can help exclude primary biliary cirrhosis.
- Patients with PSC should be tested at least once for elevated serum IgG4 levels.
- UDCA in doses >28 mg/kg/day should not be used for management of patients with PSC
- ERCP with balloon dilatation is recommended for PSC patients with dominant stricture and pruritus, and/or cholangitis, to relieve symptoms.
- PSC with a dominant stricture seen on imaging should have an ERCP with cytology, biopsies and FISH to exclude diagnosis of cholangiocarcinoma.
- PSC patients undergoing ERCP should have antibiotic prophylaxis to prevent post-ERCP cholangitis.
- Routine stenting after dilation of a dominant stricture is not required, whereas short-term stenting may be required in patients with severe stricture.
- Liver transplantation, when possible, is recommended over medical therapy or surgical drainage in PSC patients with decompensated cirrhosis, to prolong survival
- Patients should be referred for liver transplantation when their MELD score exceeds 14.
- Annual colon surveillance preferably with chromoendoscopy is recommended in PSC patients with colitis beginning at the time of PSC diagnosis.
- A full colonoscopy with biopsies is recommended in patients with PSC regardless of the presence of symptoms to assess for associated colitis at the time of PSC diagnosis.
- Some advocate repeating the exam every 3–5 years in those without prior evidence of colitis.
- Consider screening for cholangiocarcinoma with regular cross-sectional imaging with ultrasound or MR and serial CA 19-9 every 6–12 months.
- Cholecystectomy should be performed for patients with PSC and gallbladder polyps >8 mm, to prevent the development of gallbladder adenocarcinoma.
- Further testing for autoimmune hepatitis is recommended for patients <25 years of age with PSC or those with higher- than-expected levels of aminotransferases usually 5× upper limit of normal.
- MRCP is recommended for patients <25 years of age with autoimmune hepatitis, who have elevated serum ALP usually >2× the upper limit of normal.
- Local skin treatment should be performed with emollients and/or antihistamines in patients with PSC and mild pruritus, to reduce symptoms.
- Bile acid sequestrants such as cholestyramine should be taken (prescribed) in patients with PSC and moderate pruritus, to reduce symptoms. Second-line treatment such as rifampin and naltrexone can be considered if cholestyramine is ineffective or poorly tolerated.
- Recommend screening for varices in patients with signs of advanced disease with platelet counts <150×103/dl.
- Patients with PSC should undergo BMD screening at diagnosis with dual energy X-ray absorption at diagnosis and repeated at 2- to 4-year intervals.
- Patients with advanced liver disease should be screened and monitored for fat-soluble vitamin deficiencies.
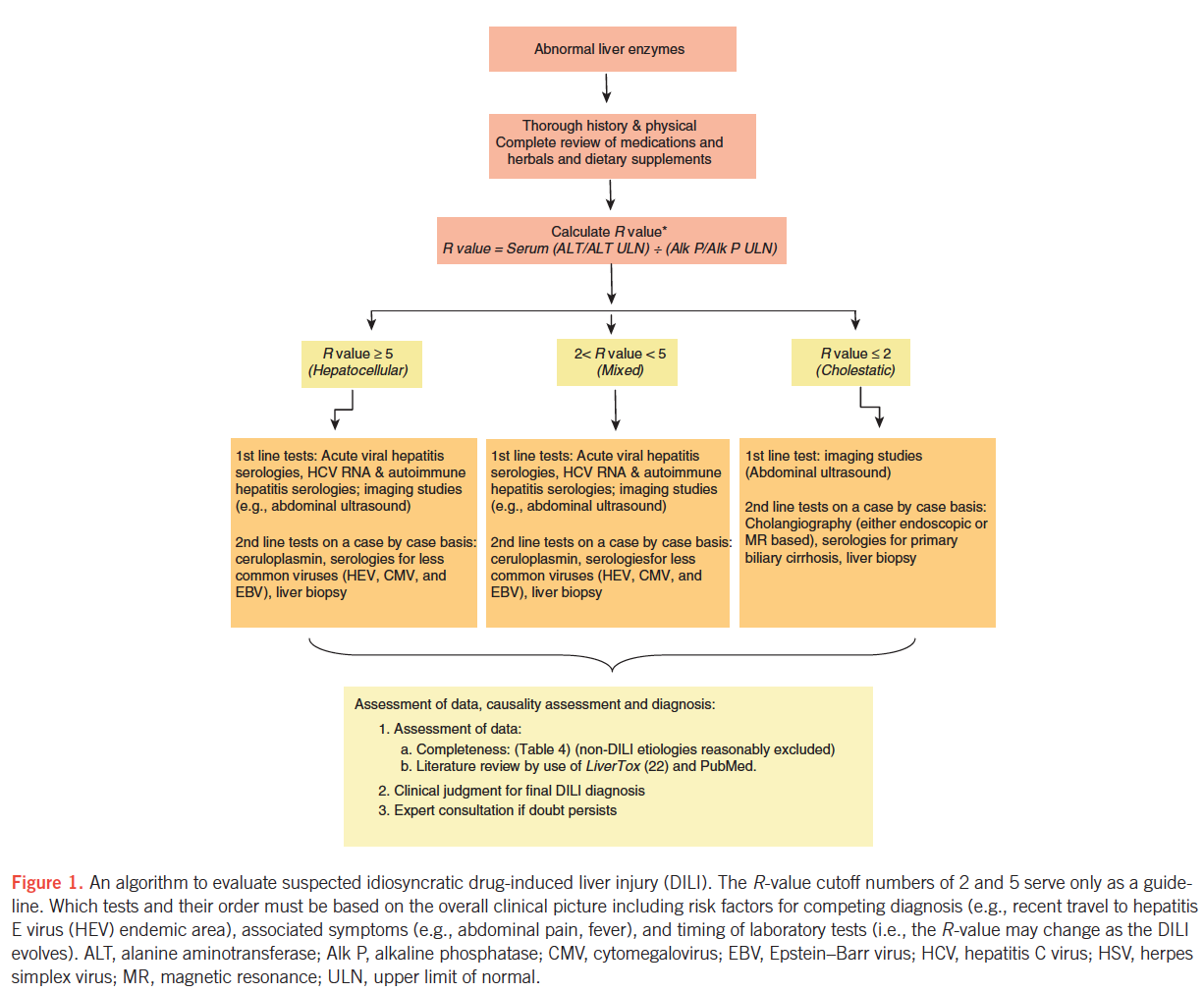
Diagnosis and Management of Idiosyncratic Drug-Induced Liver Injury
Please review the ACG Clinical Guideline on The Diagnosis and Management of Idiosyncratic Drug-Induced Liver Injury
Idiosyncratic drug-induced liver injury (DILI) is a rare adverse drug reaction and it can lead to jaundice, liver failure, or even death. Antimicrobials and herbal and dietary supplements are among the most common therapeutic classes to cause DILI in the Western world. DILI is a diagnosis of exclusion and thus careful history taking and thorough work-up for competing etiologies are essential for its timely diagnosis. In this ACG Clinical Guideline, the authors present an evidence-based approach to diagnosis and management of DILI with special emphasis on DILI due to herbal and dietary supplements and DILI occurring in individuals with underlying liver disease. Download the Guideline for your review.
Terminology and definitions
Intrinsic DILI – Hepatotoxicity with potential to affect all individuals to varying degrees. Reaction typically stereotypic and dose dependent (e.g., acetaminophen).
Idiosyncratic DILI – Hepatotoxicity affecting only rare susceptible individuals. Reaction less dose dependent and more varied in latency, presentation, and course.
Chronic DILI – Failure of return of liver enzymes or bilirubin to pre-DILI baseline, and/or other signs or symptoms of ongoing liver disease (e.g., ascites, encephalopathy, portal hypertension, coagulopathy) 6 months after DILI onset.
Latency – Time from medication (or HDS) start to onset of DILI.
Wash-out, resolution, or de-challenge – Time from DILI onset to return of enzymes and/or bilirubin to pre-DILI baseline levels.
Rechallenge – Re-administration of medication or HDS to a patient who already had a DILI to the same agent.
Hy’s law – Observation made by late Hyman Zimmerman suggesting a 1 in 10 mortality risk of DILI if the following three criteria are met:
- Serum ALT or AST > 3 × ULN
- Serum total bilirubin elevated to > 2 × ULN, without initial findings of cholestasis (elevated serum alkaline phosphatase)
- No other reason can be found to explain the combination of increased aminotransferases and bilirubin, such as viral hepatitis A, B, C, or other preexisting or acute liver disease
Temple’s corollary – An imbalance in the frequency of ALT > 3 × ULN between active treatment and control arms in a randomized controlled trial. This is used to assess for hepatotoxic potential of a drug from premarketing clinical trials
R-value – ALT/ULN ÷ AP/ULN. Used to defined hepatotoxicity injury patterns: hepatocellular (R > 5), mixed (R =2 – 5), and cholestatic (R < 2)
RUCAM – Diagnostic algorithm that uses a scoring system based on clinical data, pre-existing hepatotoxicity literature on the suspected agent and rechallenge
Variables that may predispose individuals to idiosyncratic DILI
- Host factors
- Age
- Gender
- Pregnancy
- Malnutrition
- Obesity
- Diabetes mellitus
- Co-morbidities including underlying liver disease
- Indications for therapy
- Environmental factors
- Smoking
- Alcohol consumption
- Infection and inflammatory episodes
- Drug-related factors
- Daily dose
- Metabolic profile
- Class effect and cross-sensitization
- Drug interactions and polypharmacy
Recommended minimal elements of a diagnostic evaluation in the work-up of suspected DILI
- Gender – Particularly pertinent for competing disorders (e.g., PBC)
- Age – Particularly pertinent for competing disorders (e.g., HEV)
- Race/ethnicity – Particularly pertinent for competing disorders (e.g., sarcoidosis, sickle cell-related biliary stone disease, oriental sclerosing cholangitis)
- Indication for use of drug or herbal or dietary supplement (HDS)
- Concomitant diseases – Particularly pertinent disorders may include sepsis, heart failure, hypotension episodes, recent general anesthesia, parenteral nutrition, and cancer
- Presence of rechallenge – Give timing of rechallenge if done
- History of other drug reactions – Certain cross-reactivities may exist (e.g., anti-epileptics)
- History of other liver disorders – Chronic viral hepatitis, NAFLD, hemochromatosis, alcoholic liver disease, PSC, PBC, liver cancer
- History of alcohol use – Past vs. present; estimated grams per day; sporadic vs. binge drinking vs. regular (daily or weekly)
- Exposure time (“latency”) – Start and stop dates or total number of days, weeks, or months taken
- Symptoms and signs – Presence or absence, time of onset, type (fatigue, weakness, abdominal pain, nausea, dark urine, icterus, jaundice, pruritus, fever, rash)
- Physical findings – Fever, rash, hepatomegaly, hepatic tenderness, signs of chronic liver disease
- Medications and HDS products – Complete list of medications or HDS products with particular attention to those started in the previous 6 months
- Laboratory results – Day of first abnormal liver biochemistry; liver biochemistries, eosinophil counts at presentation
- Viral hepatitis serologies – Anti-HAV IgM, HBsAg, anti-HBc IgM, anti-HCV, HCV RNA
- Auto-immune hepatitis serologies – ANA, anti-smooth muscle antibody, IgG level
- Imaging – US± Doppler, CT, or MRI ± MRCP
- Histology, if available – Timing of biopsy in relation to enzyme elevation and onset
- Washout (de-challenge) data – Follow-up liver biochemistries
- Clinical outcome – Resolution, transplant, death, and timing of each
Most common or well-described DILI agents and the patterns of their liver injury
Agent – Latency – Typical pattern of injury/identifying features (short=3-30 days; moderate=30-90 days; long > 90 days).
- Antibiotics
- Amoxicillin/clavulanate – Short to moderate – Cholestatic injury, but can be hepatocellular; DILI onset is frequently detected after drug cessation
- Isoniazid – Moderate to long – Acute hepatocellular injury similar to acute viral hepatitis
- Trimethoprim/sulfamethoxazole – Short to moderate – Cholestatic injury, but can be hepatocellular; often with immunoallergic features (e.g., fever, rash, eosinophilia)
- Fluoroquinolones – Short – Variable: hepatocellular, cholestatic, or mixed in relatively similar proportions
- Macrolides – Short – Hepatocellular, but can be cholestatic
- Nitrofurantoin
- Acute form (rare) – Short – Hepatocellular
- Chronic form – Moderate to long (months – years) – Typically hepatocellular; often resembles idiopathic autoimmune hepatitis
- Minocycline – Moderate to long – Hepatocellular and often resembles autoimmune hepatitis
- Anti-epileptics
- Phenytoin – Short to moderate – Hepatocellular, mixed, or cholestatic often with immune-allergic features (e.g., fever, rash, eosinophilia) (anti-convulsant hypersensitivity syndrome)
- Carbamazepine – Moderate – Hepatocellular, mixed, or cholestatic often with immune-allergic features (anti-convulsant hypersensitivity syndrome)
- Lamotrigine – Moderate – Hepatocellular often with immune-allergic features (anti-convulsant hypersensitivity syndrome)
- Valproate
- Hyperammonemia – Moderate to long – Elevated blood ammonia, encephalopathy
- Hepatocellular – Moderate to long – Hepatocellular
- Reye-like syndrome – Moderate – Hepatocellular, acidosis; microvesicular steatosis on biopsy
- Analgesics
- Non-steroidal anti-inflammatory agents – Moderate to long – Hepatocellular injury
- Immune modulators
- Interferon-β – Moderate to long – Hepatocellular
- Interferon-α – Moderate – Hepatocellular, autoimmune hepatitis-like
- Anti-TNF agents – Moderate to long – Hepatocellular. Can have autoimmune hepatitis features
- Azathioprine – Moderate to long – Cholestatic or hepatocellular, but can present with portal hypertension (veno-occlusive disease, nodular regenerative hyperplasia)
- Herbals and dietary supplements
- Green tea extract (catechin) – Short to moderate – Hepatocellular
- Anabolic steroids – Moderate to long – Cholestatic; likely contained as adulterants in performance-enhancing products
- Pyrrolizidne alkaloids – Moderate to long – Sinusoidal obstruction syndrome / veno-occlusive disease; contained in some teas
- Flavocoxib – Short to moderate – Mixed hepatocellular and cholestatic
- Miscellaneous
- Methotrexate (oral) – Long – Fatty liver, fibrosis
- Allopurinol – Short to moderate – Hepatocellular or mixed. Often with immune-allergic features. Granulomas often present on biopsy
- Amiodarone (oral) – Moderate to long – Hepatocellular, mixed, or cholestatic. Macrovesicular steatosis and steatohepatitis on biopsy
- Androgen-containing steroids – Moderate to long – Cholestatic. Can present with peliosis hepatis, nodular regenerative hyperplasia, or hepatocellular carcinoma
- Inhaled anesthetics – Short – Hepatocellular. May have immune-allergic features ± fever
- Sulfasalazine – Short to moderate – Mixed, hepatocellular, or cholestatic. Often with immunoallergic features
- Proton pump inhibitors – Short – Hepatocellular; very rare
DILI: Summary statements and recommendations
- Accurate clinical history related to medication exposure and the onset of liver test abnormalities should be obtained when DILI is suspected.
- DILI is a diagnosis of exclusion, and thus appropriate competing etiologies should be excluded in a systematic manner.
- On the basis of the R-value at presentation, DILI can be categorized into hepatocellular, cholestatic, or mixed types. This categorization allows testing for competing etiologies in a systematic approach.
- Liver biopsy can help confirm a clinical suspicion of DILI, provide important information regarding disease severity, and also help exclude competing causes of liver injury.
- In individuals with suspected hepatocellular or mixed DILI:
- Acute viral hepatitis (A, B, and C) and autoimmune hepatitis should be excluded with standard serologies and HCV RNA testing.
- Routine anti-hepatitis E virus IgM testing cannot be recommended owing to unclear performance characteristics of the currently available commercial tests. However, it should be considered in the setting of heightened clinical suspicion (e.g., recent travel in an endemic area).
- Testing for acute cytomegalovirus, acute Epstein-Barr virus, or acute herpes simplex virus infection should be undertaken if classical viral hepatitis has been excluded or clinical features such as atypical lymphocytosis and lymphadenopathy suggest such causes.
- Wilson’s disease and Budd-Chiari syndrome should be considered when clinically appropriate
- In individuals with suspected cholestatic DILI:
- Abdominal imaging (ultrasound or computerized tomography scan) should be performed in all instances to exclude biliary tract pathology and infiltrative processes.
- Serological testing for primary biliary cirrhosis should be limited to those with no evidence of obvious biliary tract pathology on abdominal imaging.
- Endoscopic retrograde cholangiography should be limited to instances where routine imaging is unable to exclude impacted common bile duct stones, primary sclerosing cholangitis, or pancreatico-biliary malignancy.
- When to consider a liver biopsy?
- A liver biopsy should be considered if autoimmune hepatitis remains a competing etiology and if immunosuppressive therapy is contemplated.
- A liver biopsy may be considered in the following situations:
- If there is unrelenting rise in liver biochemistries or signs of worsening liver function despite stopping the suspected off ending agent,
- If the peak alanine aminotransferase level has not decreased by > 50 % at 30 – 60 days aft er the onset in cases of hepatocellular DILI, or if the peak alkaline phosphatase has not fallen by > 50 % at 180 days in cases of cholestatic DILI despite stopping the suspected off ending agent,
- In cases of DILI where continued use or re-exposure to the implicated agent is expected,
- If liver biochemistry abnormalities persist beyond 180 days to evaluate for the presence of chronic liver diseases (CLDs) and chronic DILI.
- In general, outcomes of idiosyncratic DILI are good, with only ~ 10 % reaching the threshold of ALF (coagulopathy and encephalopathy).
- DILI that does evolve to ALF carries a poor prognosis, with 40 % requiring liver transplantation and 42 % dying of the episode. Advanced coma grade and high MELD scores are associated with bad outcomes.
- Prognostic scores to predict outcome for DILI reaching the threshold of ALF are poor or rudimentary.
- Re-exposure to a drug that is thought likely to have caused hepatotoxicity is strongly discouraged, especially if the initial liver injury was associated with significant aminotransferase elevation (for example, > 5xULN, Hy ’ s law, or jaundice). An exception to this recommendation is in cases of life-threatening situations where there is no suitable alternative.
- In individuals with suspected DILI, especially when liver biochemistries are rising rapidly or there is evidence of liver dysfunction, the suspected agent(s) should be promptly stopped.
- No definitive therapies are available either for idiosyncratic DILI with or without ALF: however, NAC may be considered in adults with early-stage ALF, given its good safety profile and some evidence for efficacy in early coma stage patients.
- NAC is not recommended for children with severe DILI leading to ALF
Herbal or dietary supplement (HDS) induced liver injury
- HDS account for an increasing proportion of DILI events in the United States, with body building and weight loss supplements being the most commonly implicated.
- The current regulation for HDS differs substantially from conventional prescription medications. Most importantly, there is no requirement for premarketing safety analyses of HDS.
- Patients and providers must be aware that regulation is not rigorous enough to assure complete safety of marketed products. Patients should be made aware of this fact, and of the potential for HDS to cause liver injury.
- Current causality assessment approaches are not well suited for HDS hepatotoxicity, given the possibility of product variability and contamination; however, expert opinion is probably the best suited for HDS hepatotoxicity, as all information is taken into consideration in assigning a likelihood of injury.
- Voluntary reporting of suspected HDS hepatotoxicity cases through the FDA MEDWATCH system is essential.
- Patients should be encouraged to report the use of HDS to their health-care providers, and be reminded that supplements are not subjected to the same rigorous testing for safety and efficacy as are prescription medications.
- The same diagnostic approach for DILI is applicable to suspected HDS hepatotoxicity. That is, other forms of liver injury must be excluded through a careful history and appropriate laboratory testing and hepatobiliary imaging. Excluding other causes, the diagnosis of HDS hepatotoxicity can be made with confidence in the setting of recent use of HDS.
- Patients with suspected HDS hepatotoxicity should stop all HDS hepatotoxicity and be monitored for resolution of their liver injury.
DILI in patients with chronic liver disease (CLD)
- There are no data to show that underlying CLD is a major risk factor for all-cause DILI, but it may increase the risk for DILI due to selected medications. Patients with chronic HBV and HCV may be more prone to develop liver injury due to specific agents such as isoniazid and antiretrovirals, and may experience more severe outcomes.
- Individuals with underlying fatty liver disease are not at an increased risk for hepatotoxicity from statins.
- The diagnosis of DILI in patients with CLD requires a high index of suspicion and exclusion of other more common causes of acute liver injury, including a flare-up of the underlying liver disease.
- The use of potentially hepatotoxic drugs in CLD patients should be based upon the risk versus benefit of the proposed therapy on a case-by-case basis.
- There are no data to recommend a specific liver biochemistry monitoring plan when a potential hepatotoxic agent is prescribed in individuals with known CLD. Often, information contained in the package inserts is incomplete or unhelpful. Patients should be advised to promptly report any new-onset symptoms such as scleral icterus, abdominal pain / discomfort, nausea / vomiting, pruritis, or choluria. In addition, it is reasonable to monitor serum liver biochemistries at 4 – 6 week intervals, especially during the initial 6 months of treatment with a potentially hepatotoxic agent.
In Summary
- In individuals with suspected hepatocellular or mixed DILI:
- Acute viral hepatitis (A, B, and C) and auto-immune hepatitis should be excluded with standard serologies and HCV RNA testing.
- Anti-HEV IgM testing cannot be recommended because of unclear performance characteristics of the currently available commercial tests. However, it should be considered in the setting of heightened clinical suspicion (e.g., recent travel in an endemic area).
- Testing for acute CMV, acute EBV, or acute HSV infection should be undertaken if classical viral hepatitis has been excluded or clinical features such as atypical lymphocytosis, lymphadenopathy suggest such causes.
- Wilson’s disease and Budd-Chiari syndrome should be considered when clinically appropriate.
- In individuals with suspected cholestatic DILI:
- Abdominal imaging (ultrasound or CT scan) should be performed in all instances to exclude biliary tract pathology and infi ltrative processes.
- Serological testing for primary biliary cirrhosis should be limited to those with no evidence of obvious biliary tract pathology on abdominal imaging.
- Endoscopic retrograde cholangiography should be limited to instances where routine imaging is unable to exclude impacted common bile duct stones, primary sclerosing cholangitis, or pancreatico-biliary malignancy.
- When to consider a liver biopsy?
- A liver biopsy should be considered if autoimmune hepatitis remains a competing etiology and if immunosuppressive therapy is contemplated.
- A liver biopsy may be considered:
- If there is unrelenting rise in liver biochemistries or signs of worsening liver function despite stopping the suspected offending agent.
- If peak ALT level has not fallen by > 50 % at 30 – 60 days after onset in cases of hepatocellular DILI, or if peak Alk P has not fallen by > 50 % at 180 days in cases of cholestatic DILI despite stopping the suspected offending agent.
- In cases of DILI where continued use or re-exposure to the implicated agent is expected.
- If liver biochemistry abnormalities persist beyond 180 days to evaluate for the presence of chronic liver diseases and chronic DILI.
- Re-exposure to a drug thought likely to have caused hepatotoxicity is strongly discouraged, especially if the initial liver injury was associated with significant aminotransferase elevation (e.g., > 5xULN, Hy’s law), or jaundice. An exception to this recommendation is in cases of life-threatening situations where there is no suitable alternative.
- In individuals with suspected DILI, especially when liver biochemistries are rising rapidly or there is evidence of liver dysfunction, suspected agent(s) should be promptly stopped.
- No definitive therapies are available either for idiosyncratic DILI with or without ALF: however, NAC may be considered in adults with early-stage ALF, given its good safety profile and some evidence for efficacy in early coma stage patients.
- NAC is not recommended for children with severe DILI leading to ALF.
- Patients should be encouraged to report use of HDS to their health-care providers, and be reminded that supplements are not subjected to the same rigorous testing for safety and efficacy as are prescription medications.
- The same diagnostic approach for DILI is applicable to suspected HDS-hepatotoxicity. That is, other forms of liver injury must be excluded through a careful history, and appropriate laboratory testing and hepatobiliary imaging. Excluding other causes, the diagnosis of HDS-hepatotoxicity can be made with confidence in the setting of recent use of HDS.
- Patients with suspected HDS-hepatotoxicity should stop all HDS-hepatotoxicity and be monitored for resolution of their liver injury.
- The diagnosis of DILI in patients with CLD requires a high index of suspicion and exclusion of other more common causes of acute liver injury including a flare-up of the underlying liver disease.
- The use of potentially hepatotoxic drugs in CLD patients should be based upon the risk vs. benefit of the proposed therapy on a case-by-case basis.
- There are no data to recommend a specific liver biochemistry monitoring plan when a potential hepatotoxic agent is prescribed in individuals with known CLD. Often, information contained in the package inserts is incomplete or unhelpful. Patients should be advised to promptly report any new onset symptoms such as yellowing of their eyes, abdominal pain / discomfort, nausea / vomiting, itching, or dark urine. In addition, it is reasonable to monitor serum liver biochemistries at 4 – 6 weekly intervals, especially during the initial 6 months of treatment with a potentially hepatotoxic agent.
Am J Gastroenterol advance online publication, 17 June 2014; doi: 10.1038/ajg.2014.131
Abbreviations:
ALF, acute liver failure;
Alk P, alkaline phosphatase;
ALT, alanine aminotransferase;
ANA, anti-nuclear antibody;
AP, alkaline phosphatase;
AST, aspartate aminotransferase;
CLD, chronic liver disease
CMV, cytomegalovirus;
CT, computerized tomography;
DILI, drug-induced liver injury;
EBV, Epstein-Barr virus;
HAV, hepatitis A virus;
HBc, hepatitis B core antigen;
HBs, hepatitis B surface antigen;
HCV, hepatitis C virus;
HDS, herbal or dietary supplement;
HEV, hepatitis E virus;
HSV, herpes simplex virus;
NAC, N-acetyl cysteine:
NAFLD, nonalcoholic fatty liver disease;
PBC, primary biliary cirrhosis;
PSC, primary sclerosing cholangitis;
Ig, immunoglobulin;
MRI, magnetic resonance imaging;
MRCP, magnetic resonance cholangiopancreatography;
RUCAM, Roussel Uclaf Causality Assessment Method;
TNF, tumor necrosis factor;
ULN, upper limit of normal.
US, ultrasound.
The Diagnosis and Management of Focal Liver Lesions
- An MRI or triple-phase CT should be obtained in patients with cirrhosis with an ultrasound showing a lesion of >1cm.
- Patients with chronic liver disease, especially with cirrhosis, who present with a solid FLL are at a very high risk for having HCC and must be considered to have HCC until otherwise proven.
- A diagnosis of HCC can be made with CT or MRI if the typical characteristics are present: a solid FLL with enhancement in the arterial phase with washout in the delayed venous phase should be considered to have HCC until otherwise proven.
- If an FLL in a patient with cirrhosis does not have typical characteristics of HCC, then a biopsy should be performed in order to make the diagnosis.
- MRI or CT should be obtained if CCA is suspected clinically or by ultrasound.
- A liver biopsy should be obtained to establish the diagnosis of CCA if the patient is non operable.
Suspected hepatocellular adenoma
- Oral contraceptives, hormone-containing IUDs, and anabolic steroids are to be avoided in patients with hepatocellular adenoma.
- Obtaining a biopsy should be reserved for cases in which imaging is inconclusive and biopsy is deemed necessary to make treatment decisions.
- Pregnancy is not generally contraindicated in cases of hepatocellular adenoma < 5 cm and an individualized approach is advocated for these patients.
- In hepatocellular adenoma ≥ 5 cm, intervention through surgical or nonsurgical modalities is recommended, as there is a risk of rupture and malignancy.
- If no therapeutic intervention is pursued, lesions suspected of being hepatocellular adenoma require follow-up CT or MRI at 6- to 12-month intervals. The duration of monitoring is based on the growth patterns and stability of the lesion over time.
- Clinical variants of hepatocellular adenoma
- Liver adenomatosis.
- Multiple adenomas, defined as between > 3 and ≥ 10 lesions, are collectively referred to as liver adenomatosis. These multiple lesions have identical clinical, histological, and radiographic features as hepatocellular adenomas and are managed in the same manner.
- Telangiectatic hepatocellular adenoma
- Previously known as telangiectatic focal nodular hyperplasia, telangiectatic hepatocellular adenoma (THCA) has recently been reclassified as a subcategory of inflammatory hepatocellular adenoma. THCA should be managed as aggressively as hepatocellular adenomas as they are likely to be symptomatic, prone to hemorrhage, and may contain focal areas of necrosis. The high likelihood of hemorrhage combined with an unknown potential of transformation to HCC makes surgery the recommended treatment.
- Liver adenomatosis.
Suspected hemangioma
- An MRI or CT scan should be obtained to confirm a diagnosis of hemangioma.
- Liver biopsy should be avoided if the radiologic features of a hemangioma are present.
- Pregnancy and the use of oral contraceptives or anabolic steroids are not contraindicated in patients with a hemangioma.
- Regardless of the size, no intervention is required for asymptomatic hepatic hemangiomas. Symptomatic patients with impaired quality of life can be referred for surgical or nonsurgical therapeutic modalities by an experienced team.
Suspected focal nodular hyperplasia
- An MRI or CT scan should be obtained to confirm a diagnosis of FNH. A liver biopsy is not routinely indicated to confi rm the diagnosis.
- Pregnancy and the use of oral contraceptives or anabolic steroids are not contraindicated in patients with FNH.
- Asymptomatic FNH does not require intervention.
- Annual US for 2-3 years is prudent in women diagnosed with FNH who wish to continue OCP use. Individuals with a firm diagnosis of FNH who are not using OCP do not require follow-up imaging.
- Liver biopsy is required to confirm the diagnosis of NRH.
- Pregnancy and the use of oral contraceptives or anabolic steroids are not contraindicated in patients with an NRH.
- Asymptomatic NRH does not require intervention.
- Management of NRH is based on diagnosing and managing any underlying predisposing disease processes.
- A hepatic cyst identified on US with septations, fenestrations, calcifications, irregular walls, or daughter cysts should prompt further evaluation with a CT or MRI.
- Asymptomatic simple hepatic cysts should be observed with expectant management.
- Aspiration of asymptomatic, simple hepatic cysts is not recommended.
- Symptomatic simple hepatic cysts may be managed with laparoscopic deroofing rather than aspiration and sclerotherapy, dictated based on availability of local expertise.
- Routine fluid aspiration is not recommended when BCA is suspected because of limited sensitivity and the risk of malignant dissemination.
- Imaging characteristics suggestive of BC or BCA, such as internal septations, fenestrations, calcifications, or irregular walls, should lead to referral for surgical excision.
- Complete surgical excision, by an experienced team, is recommended if BC or BCA is suspected.
- Routine medical therapy with mammalian target of rapamycin inhibitors or somatostatin analogs is not recommended.
- Aspiration, deroofing, resection of a dominant cyst(s) can be performed based on the patient’s clinical presentation and underlying hepatic reserve.
- Liver transplantation with or without kidney transplantation can be considered in patients with refractory symptoms and significant cyst burden.
- MRI is preferred over CT for concomitant evaluation of the biliary tree and cystic contents.
- Monotherapy with antihelminthic drugs is not recommended in symptomatic patients who are surgical or percutaneous treatment candidates.
- Adjunctive therapy with antihelminthic therapy is recommended in patients undergoing PAIR or surgery, and in those with peritoneal rupture or biliary rupture.
- Percutaneous treatment with PAIR is recommended for patients with active hydatid cysts who are not surgical candidates, who decline surgery, or who relapse after surgery.
- Surgery, either laparoscopic or open, based on available expertise, is recommended in complicated hydatid cysts with multiple vesicles, daughter cysts, fistulas, rupture, hemorrhage, or secondary infection.

Am J Gastroenterol advance online publication, 19 August 2014; doi: 10.1038/ajg.2014.213
- Heterogeneous; hyperechoic if steatotic but anechoic center if hemorrhage
- Well demarcated with peripheral enhancement; homogenous more often than heterogeneous; hypodense if steatotic, hyperdense if hemorrhagic
- HNF1 α : signal lost on chemical shift; moderate arterial enhancement without persistent enhancement during delayed phase
- IHCA: markedly hyperintense on T2 with stronger signal peripherally; persistent enhancement in delayed phase
- β – Catenin: inflammatory subtype has same appearance as IHCA; noninflammatory is heterogeneous with no signal dropout on chemical shift, isointense of T1 and T2 with strong arterial enhancement and delayed washout
- Variable appearance
- Hypo- to isoattenuating
- T1: heterogeneous and well-defined iso- to hyperintense mass. Strongly hyperintense with persistent contrast enhancement in delayed phase
- Hyperechoic with well-defined rim and with few intranodular vessels
- Discontinuous peripheral nodular enhancement isoattenuating to aorta with progressive centripetal fi ll-in
- T1: hypointense; discontinuous peripheral enhancement with centripetal fi ll-in
- T2: hyperintense relative to spleen
- Generally isoechoic
- Central scar. Arterial phase shows homogenous hyperdense lesion; returns to pre contrast density during portal phase that is hypo- or isodense
- T1: isointense or slightly hypointense. Gadolinium produces early enhancement with central scar enhancement during delayed phase
- T2: slightly hyperintense or isointense
- Isoechoic / hyperechoic
- Nonenhancing nodules, sometimes hypodense, with variable sizes (most sub-centimeter)
- T1: hyperintense
- T2: varied intensity (hypo / iso / hyperintense)
- Anechoic, homogeneous,fluid filled. Smooth margins
- Well-demarcated, water-attenuated, smooth lesion without an internal structure. No enhancement with contrast
- Well-defined, homogeneous lesion. No enhancement with contrast.
- T1: hypointense signal intensity
- T2: hyperintense signal intensity
- Irregular walls, internal septations forming loculi
- Heterogeneous septations, internal septations, irregular papillary growths, thickened cyst walls
- May appear heterogeneous.
- T1: Hypointense signal intensity
- T2: Hyperintense signal intensity
- Multiple hepatic cysts, similar in characteristics to SHC US findings
- Multiple hepatic cysts, similar in characteristics to SHC CT findings
- Multiple hepatic cysts, similar in characteristics to SHC MRI findings
- May appear similar to SHC. Progress to develop thick, calcified walls, hyperechoic / hypoechoic contents. Daughter cysts in periphery.
- Hypodense lesion with hypervascular pericyst wall, distinct endocyst wall. Calcified walls and septa easily detected. Daughter cysts seen peripherally within mother cyst.
- T1: Hypointense signal intensity of cyst contents.
- T2: Hyperintense signal intensity of cyst contents.
- Hypointense rim on T2.
- Daughter cysts seen peripherally within mother cyst. Collapse parasitic membranes seen as floating linear structures within cyst.
Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis
The World Gastroenterology Organization (WGO) Global Guidelines published guidelines on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis in the July issue of the Journal of Clinical Gastroenterology.
- Suspected NAFLD involves central obesity, diabetes mellitus, dyslipidemia, metabolic syndrome, abnormal liver function tests, and/or ultrasound changes consistent with fatty liver.
- Minimal assessment should include
- bilirubin
- alanine aminotransferase
- aspartate aminotransferase
- g-glutamyl transferase
- albumin
- fasting serum lipids
- complete blood count
- hepatitis C virus
- hepatitis B surface antigen
- antinuclear antibody
- fasting blood glucose
- oral glucose tolerance test if fasting blood glucose level of 5.6 mmol/L or higher
- height, weight, body mass index, waist circumference
- blood pressure
- abdominal ultrasound
- Optional tests include
- abdominal computed tomography if uninformative ultrasound
- liver biopsy if diagnostic uncertainty or for patients at risk for advanced hepatic fibrosis.
- Additional tests include tests for
- hereditary hemochromatosis
- Wilson’s disease
- alpha-1 antitrypsin deficiency
- polycystic ovary syndrome
- autoimmune liver diseases
WGO SUMMARY STATEMENT
- NAFLD and NASH represent a major global public health problem, which is pandemic and affects rich and poor countries alike.
- There is insufficient evidence to justify screening for NASH/advanced liver disease in the general population.
- The diagnosis should be sought in all patients who present with risk factors for NASH.
- Not all patients with risk factors will have NAFLD or NASH, and not all patients with NASH will have standard risk factors.
- Not every person with fatty liver needs aggressive therapy.
- Diet and exercise should be instituted for all patients.
- Liver biopsy should be reserved for those patients who have risk factors for NASH and/or other liver diseases.
- Patients with NASH or risk factors for NASH should first be treated with diet and exercise. Vitamin E or pentoxifylline may be added in these patients. Experimental therapy should be considered only in appropriate hands and only in patients who fail to achieve a 5% to 10% weight reduction over 6 months to 1 year of successful lifestyle changes.
- Bariatric surgery should be considered in patients in whom the above approaches fail, and it should be performed before the patient becomes cirrhotic.
- Liver transplantation is successful in patients who meet the criteria for liver failure; however, NASH may recur after transplantation and is likely to be denied to patients with morbid obesity.
- NAFLD and NASH are also becoming an increasingly serious problem in pediatric patients, including those under the age of 10.
Ultimately, NAFLD and NASH are diagnoses of exclusion and require careful consideration of other diagnoses. Just as the clinician cannot diagnose NASH on the basis of clinical data alone, the pathologist can document the histologic lesions of steatohepatitis, but cannot reliably distinguish those of nonalcoholic origin from those of alcoholic origin.
HCV Treatment Guidelines
The American Association for the Study of Liver Diseases (AASLD) and the Infectious Disease Society of America (IDSA) published guidelines for the treatment of HCV. These HCV Treatment Guidelines will be published in hard copy in Hepatology and in the Journal of Infectious Diseases. The full report can already be accessed as a PDF file.
Detailed discussions guide the clinician according to the HCV genotype, past treatment failures or responses, and interferon ineligibility.
Some important points to remember: Patients receiving antiviral therapy require careful pretreatment assessment for comborbidities that may influence treatment response. All patients should have careful monitoring during treatment, particularly for anemia if ribavirin is included in the regimen. Some regimens should be considered only in those patients who require immediate treatment, as it is anticipated that safer and more effective IFN-free regimens will become available by 2015.
1. Regimens are classified as either
- “Recommended” when it is favored for most patients or
- “Alternative” when optimal in a particular subset of patients in that category, or
- “Not Recommended” when a treatment is clearly inferior or is deemed harmful. Such regimens should not be administered to patients with HCV infection.
2. Interferon ineligible is defined as one or more:
- Intolerance to IFN
- Autoimmune hepatitis and other autoimmune disorders
- Hypersensitivity to PEG or any of its components
- Decompensated hepatic disease
- History of depression, or clinical features consistent with depression
- A baseline neutrophil count below 1500/μL, a baseline platelet count below 90,000/μL or baseline hemoglobin below 10 g/dL
- A history of preexisting cardiac disease
3. Specific considerations are addressed in other sections of the document:
- HIV/HCV coinfection
- Compensated and decompensated cirrhosis (moderate or severe hepatic impairment)
- Post-liver transplant HCV
- Patients with severe renal impairment or ESRD
A) INITIAL TREATMENT OF HCV INFECTION IN PATIENTS STARTING TREATMENT for
This section provides guidance on the recommended initial treatments for persons with chronic HCV infection who are naive to HCV treatment or who have achieved an undetectable level of virus during a prior treatment course of PEG/RBV and relapsed (relapsers) according to genotype.
- Genotype 1
- Genotype 2
- Genotype 3
- Genotype 4
- Genotype 5 or 6
A Summary Table of Recommendations for patients who are initiating therapy for HCV infection or who experienced relapse after prior PEG/RBV therapy by HCV genotype is provided.
This section provides guidance on the retreatment of a person with chronic HCV infection in whom prior therapy has failed, addressing non-responders, which includes null responders (those in whom serum HCV RNA levels declined less than 2 log10 IU/mL by week 12 during a prior treatment course) and partial responders according to genotype.
- Genotype 1
- Genotype 2
- Genotype 3
- Genotypes 4, 5 and 6
A Summary Table of Recommendations for patients in whom previous PEG/RBV treatment has failed is provided.
C) UNIQUE PATIENT POPULATIONS ARE FURTHER ADDRESSED:
The recommendations are a MUST-READ for all providers who care for patients with HCV infection.
